This chapter should be cited as follows:
Ching SOH, Ip PPC, Glob Libr Women's Med
ISSN: 1756-2228; DOI 10.3843/GLOWM.421963
The Continuous Textbook of Women’s Medicine Series – Gynecology Module
Volume 13
Gynecological cancer
Volume Editors:
Professor Hextan Ngan, Department of Obstetrics and Gynaecology, The University of Hong Kong, Hong Kong
Professor Karen Chan, Department of Obstetrics and Gynaecology, The University of Hong Kong, Hong Kong
Chapter
Endometrial Cancer Pathology
First published: May 2026
Study Assessment Option
By answering four multiple-choice questions (randomly selected) after studying this chapter, readers can qualify for Continuing Professional Development points plus a Study Completion Certificate from GLOWM.
See end of chapter for details.

INTRODUCTION
Endometrial carcinoma is one of the commonest gynecologic cancers in high-income countries,1,2,3,4 with the highest incidence being in North America.5 Traditionally, it has been classified into histological subtypes based on morphology, as reflected in the World Health Organization (WHO) Classification of Tumours.6 In a landmark paper published in 2013 in Nature, The Cancer Genome Atlas (TCGA) proposed a new molecular classification with prognostic significance,7 which has gradually been incorporated into clinical practice.
EPIDEMIOLOGY
The peak incidence of endometrial carcinoma occurs in the 7th to 8th decades.2 The worldwide incidence has increased by over 130% in the past 30 years,5 with largest increase observed in South Africa and several countries in Asia.3 The disease-associated mortality in the USA is rising by an average of 2.5% annually.4,8
The major risk factors for endometrial carcinoma include conditions associated with estrogen excess, such as obesity, endogenous estrogen exposure from early menarche and polycystic ovarian syndrome, chronic anovulation, late menopause, exogenous estrogen replacement therapy and tamoxifen therapy.2,5 Patients with genetic syndromes, including Lynch syndrome and Cowden syndrome, also have increased risk for endometrial carcinomas.5 High-grade carcinomas are associated with lower body mass index (BMI), parity, African ethnicity and a personal history of breast cancer.2
CLINICAL FEATURES
The commonest presentation is abnormal uterine bleeding, including postmenopausal bleeding. The prevalence of post-menopausal bleeding among patients with endometrial cancer is around 90%.9 Most patients are diagnosed at an early stage when disease is confined to the uterus. Advanced disease may present with pelvic or abdominal symptoms resembling those of ovarian carcinoma, including pelvic or abdominal pain and a mass lesion,2,10 and they may present with distant metastases.10
CLASSIFICATION OF ENDOMETRIAL CARCINOMAS
Historically, endometrial carcinoma was classified into two distinct types. Type I was estrogen-related, occurred in obese or metabolically disturbed women and was histologically low-grade, with a favorable prognosis. In contrast, Type II was usually not associated with estrogen, occurred in non-obese women with atrophic endometrium and included high-grade histologies such as serous and clear cell carcinomas, with a poorer prognosis.10 However, these categories show significant overlap in clinical, pathological and molecular features, and the histological diagnosis of high-grade carcinomas shows considerable interobserver variability.11,12 As such, classification of endometrial carcinomas according to these two subtypes is no longer recommended as a formal classification system. In the ensuing decades, endometrial carcinomas were classified primarily according to microscopic architecture and cellular features,13,14 which formed the basis of the first four editions of the World Health Organization (WHO) Blue Books published in 1973,15 1994,16 200317 and 2014.18 Diagnostic entities in the current, 5th edition of the WHO Classification of Female Genital Tumours are primarily histology-based, with incorporation of biomarker expression, and include:10
- Endometrioid carcinoma
- Serous carcinoma
- Clear cell carcinoma
- Undifferentiated and dedifferentiated carcinomas
- Mixed carcinoma
- Other endometrial carcinomas (mesonephric-like adenocarcinoma, squamous cell carcinoma and mucinous carcinoma (gastrointestinal type))
- Carcinosarcoma
In the forthcoming 6th edition of the WHO Classification of Female Genital Tumours, in the chapter on epithelial tumors of the uterine corpus, mesonephric-like adenocarcinoma will be recognized as a standalone entity.
The histology-based diagnostic entities often share overlapping microscopic features and may result in considerable interobserver diagnostic variability. More importantly, they do not provide information on biological behavior or precise prognosis, which is essential to treatment. These will be explained in detail in the following sections.
HISTOPATHOLOGICAL GRADING
Grading is prognostically significant for endometrioid carcinomas and is conducted according to the International Federation of Gynecology and Obstetrics (FIGO) system. A grade is assigned by determining the percentage of non-squamous and non-morular solid glandular components.19 The presence of severe cytological atypia in more than 50% of tumor cells raises the grade by one level.
Historically, the system has been three-tiered:20,21
- Grade 1: tumors with ≤ 5% solid growth
- Grade 2: tumors with 6–50% solid growth
- Grade 3: tumors with > 50% solid growth
A binary grading system has now been adopted, in which Grade 1 and 2 tumors are classified as low-grade, and Grade 3 as high-grade.19 This updated system has demonstrated similar or improved prognostic performance and interobserver reproducibility.19,21 A three-tier grading system remains relevant in the setting of endometrial biopsies from women who wish to remain fertile. Non-endometrioid carcinomas, including serous, clear cell, undifferentiated and dedifferentiated carcinoma, carcinosarcoma, mesonephric-like carcinoma, neuroendocrine carcinoma, endometrial carcinoma with somatically derived germ cell components, gastric (gastrointestinal)-type endometrial carcinoma, and pilomatrix-like high-grade endometrioid carcinoma are considered high-grade tumors, by definition.
MOLECULAR CLASSIFICATION
Based on genomic characterization, endometrial cancers are classified into four groups: POLE ultramutated (good prognosis), mismatch repair (MMR) deficient (microsatellite instability hypermutated, intermediate prognosis), no specific molecular profile (low–copy-number alterations, intermediate prognosis) and p53 abnormal (high–copy-number alterations, poor prognosis)7,10 (Figure 1). This approach enables better prognostication22 (Figure 2), especially in high-grade (Grade 3) endometrial carcinomas,23 and has been endorsed by the International Society of Gynecological Pathologists21,24 (Table 1) (Figure 3).
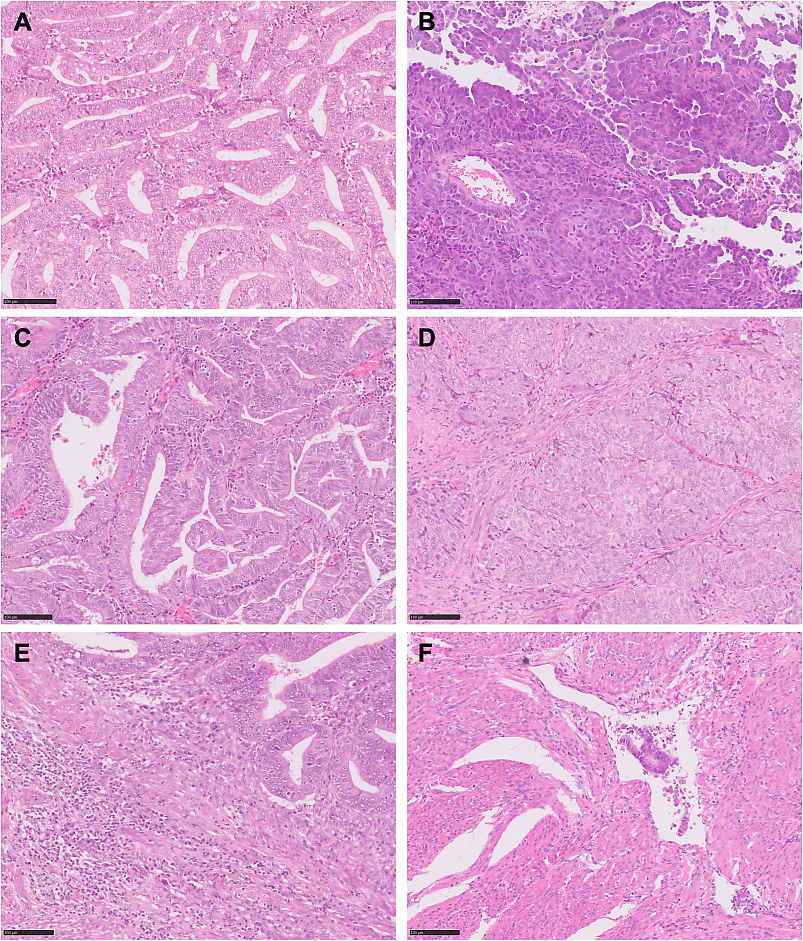
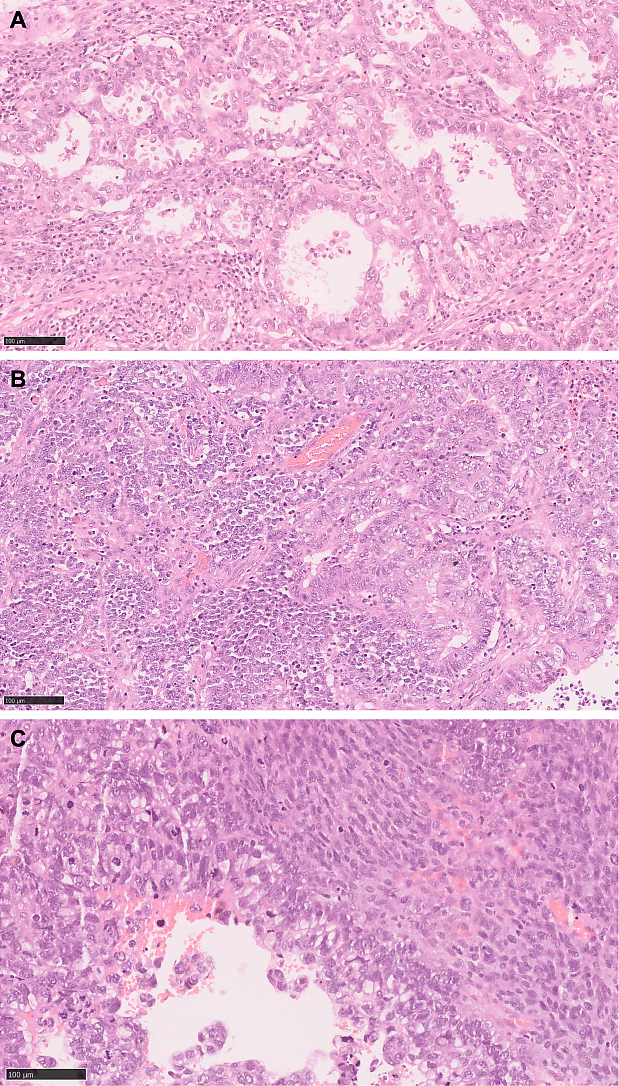
1
Histological features of endometrial carcinoma according to molecular subtypes. (A) Low-grade endometrioid carcinoma, no specific molecular profile (NSMP). The columnar tumor cells form back-to-back crowded glands with wide-open lumens and a smooth luminal border. (B) p53 abnormal endometrial serous carcinoma. Complex papillary structures covered by highly stratified tumor cells and forming slit-like spaces between them. (C) POLE-ultramutated low-grade endometrioid carcinoma. This tumor is histologically indistinguishable from other low-grade endometrioid carcinomas of other molecular subtypes. (D) POLE-ultramutated high-grade endometrioid carcinoma. Solid sheets of tumor cells with severe nuclear pleomorphism. (E) Mismatch repair-deficient low-grade endometrioid carcinoma. There is a striking lymphocytic infiltrate at the tumor infiltrating front. (F) Endometrioid carcinoma, NSMP, with extensive lymphovascular space invasion. Tumor glands admixed with fibrin and red blood cells are found inside clear spaces lined by endothelial cells. Scale bar represents 100 μm.
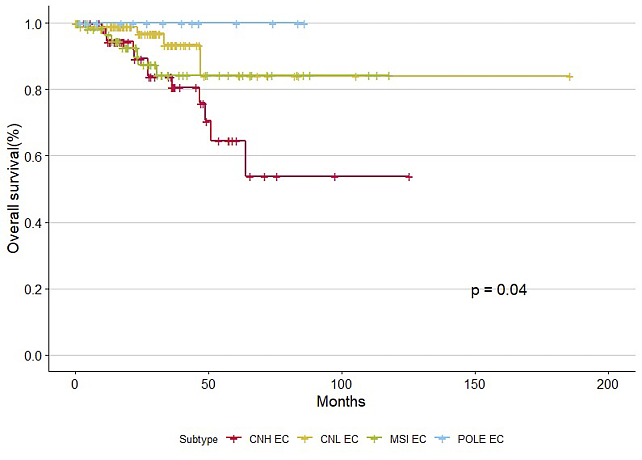
2
Kaplan–Meier survival curves of four molecular subtypes of endometrial carcinoma. POLE-ultramutated endometrial carcinoma (POLE EC) has excellent prognosis, in contrast to p53 abnormal endometrial carcinoma (CNH EC), which has the worse outcome. Mismatch repair-deficient endometrial carcinoma (MSI EC) and endometrial carcinoma of no specific molecular profile (CNL EC) have intermediate prognosis. Data generated from publicly available data of 373 endometrial cancer samples from TCGA Program.25
1
Molecular classification according to The Cancer Genome Atlas (TCGA).
Subtype | Prevalence | Molecular features | Histological features | Prognosis |
POLE ultramutated | 5–10% of endometrioid carcinomas7 | Associated with good prognosis7 | ||
Mismatch repair (MMR) deficient | Around 1/3 of endometrioid carcinomas,7 associated with Lynch syndrome in 3% of cases30 |
|
|
|
p53 abnormal | Around 10% of endometrioid carcinomas7 | Poor prognosis7 | ||
No specific molecular profile (NSMP) | 50–70% of endometrioid carcinomas7 |
|
| Intermediate prognosis7 |
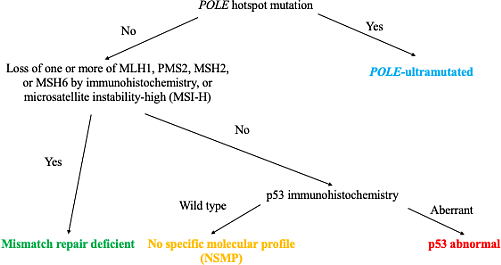
3
International Society of Gynecological Pathologists’ recommendation for molecular classification of endometrial carcinoma achieved through molecular analysis for POLE hotspot mutations, mismatch repair deficient immunohistochemistry or microsatellite instability testing, and p53 immunohistochemistry.24
Approximately 5% of tumors possess more than one molecular feature (e.g. POLE ultramutated and p53 abnormal, or MMR deficient and p53 abnormal) and are considered multiple classifiers, and these generally retain the expected prognosis associated with POLE or MMR deficiency, respectively.40
HISTOPATHOLOGICAL TYPES OF ENDOMETRIAL CARCINOMA
Endometrioid carcinoma of the uterine corpus
Endometrioid carcinoma is the most common type, accounting for approximately 80% of cases.41 It is typically preceded by endometrial atypical hyperplasia, which shares similar molecular alterations, and is associated with prolonged exposure to unopposed estrogen.10 Macroscopically, tumors may be exophytic or diffusely infiltrative, with areas of necrosis and hemorrhage.
Histologically, common architectural patterns include confluent glandular, cribriform and complex papillary structures. The neoplastic glands tend to have smooth luminal contours lined by columnar cells.42 Most tumors typically have mild to moderate nuclear atypia, enlarged and round nuclei, coarse chromatin and prominent nucleoli (Figures 1A, C and D). When a tumor is architecturally low grade, but the tumor cells have severe nuclear atypia, further investigations are crucial to exclude an aggressive endometrial carcinoma.37 Presence of mitotic figures is not a diagnostic feature of malignancy. Similar to non-neoplastic endometrium, a variety of metaplastic changes are observed in endometrioid carcinoma. They include syncytial papillary change, secretory change, hobnail, eosinophilic, ciliated cell, tubal, mucinous, morular and squamous metaplasias.10
Serous carcinoma of the uterine corpus
Serous carcinomas constitute about 10% of endometrial carcinomas but account for 40% of recurrent cases and deaths.43 Most patients present with postmenopausal vaginal bleeding, and approximately 40–50% of patients develop extrauterine metastases in surgically staged cases.43,44 They are associated with personal history of breast cancer, tamoxifen use45 and pelvic irradiation,46 with possible association with germline BRAC1/2 mutations.47 The hallmark molecular feature is TP53 mutations,7 leading to inactivation of the tumor suppressor gene.48 It is important to note that not all endometrial carcinomas with TP53 mutations are classified as serous carcinomas. Histologically, endometrioid carcinoma, including low-grade endometrioid carcinoma, clear cell carcinoma and carcinosarcoma may also harbor TP53 mutations.37,49,50,51
Serous carcinomas often arise in atrophic endometrium or endometrial polyps of postmenopausal women.44 Tumor cells form complex papillary or glandular structures, with irregular, elongated glands and slit-like luminal spaces. Cytological atypia and nuclear pleomorphism is usually significant (Figure 1B). Multinucleation and calcifications are identified in some serous carcinomas.52
Localized disease has a relatively better prognosis, but cases with extrauterine metastases (including those with coexistent serous endometrial intraepithelial carcinoma and minimally invasive disease) have poorer outcomes with increased risk of death.44 HER2 overexpression/gene amplification occurs in 25–30% of cases,53 and the addition of trastuzumab (anti-HER2 antibody) in combination with conventional chemotherapy regimen has been shown to improve survival in HER2-positive serous carcinoma of the uterine corpus.54
Clear cell carcinoma of the uterine corpus
Accounting for < 10% of endometrial carcinomas,55 clear cell carcinomas have no distinct specific molecular profile but show considerable overlap with endometrioid and serous carcinomas.56,57
Clear cell carcinomas are characterized histologically by tubulocystic, papillary and solid architectures, with short, rounded papillae often associated with hyalinized stroma.49,58,59 The neoplastic cells commonly display cuboidal, flat, polygonal or hobnail morphology with clear to eosinophilic cytoplasm. They show variable nuclear pleomorphism, typically with at least focal areas with moderate to severe nuclear atypia. Frequent nuclear stratification, cellular tufting and detached budding are absent or, at most, focally found.58,59 Mitotic activity is variable (Figure 4A). As other types of high-grade endometrial carcinoma may contain clear cells, strict adherence to architectural and cytological criteria for diagnosis is important for accurate diagnosis.59,60 On immunohistochemistry, the tumor cells are positive for Napsin A (56–93%) and AMACR (75–88%),49 and ER and PR are negative or only focally expressed.59 The four markers should be used as a panel as non-specific staining may occur with Napsin A.
4
Histological features of clear cell carcinoma, dedifferentiated carcinoma and carcinosarcoma. (A) Clear cell carcinoma of the uterus is identical to its ovarian counterpart. In the tubulocystic pattern, the lining epithelium is an admixture of hobnail and clear cells. (B) Dedifferentiated endometrial carcinoma contains a component of well-formed glands juxtaposed to discohesive sheets of epithelioid carcinoma cells (seen in left part of image). (C) Carcinosarcoma is composed of a high-grade adenocarcinoma and malignant spindle cells (seen in right part of image). Scale bar represents 100 μm.
The 5-year survival rate for clear cell carcinomas ranges from 55% to 79%.49 All four molecular subgroups are represented in clear cell carcinoma, with NSMP and p53-abnormal subgroups being more common.50,57 Older age and advanced stage correlate with poorer prognosis,58 and patients with MMR-deficient tumors tend to have better survival rate.61
Mesonephric-like carcinoma of the uterine corpus
A rare type of tumor, there is a paucity of epidemiological data for mesonephric-like carcinoma of the uterine corpus. Most patients are postmenopausal, and > 50% of cases are diagnosed at advanced stage (FIGO Stage II–IV).62,63 They share histological and immunohistochemical similarities with mesonephric and mesonephric-like carcinomas located elsewhere in the female genital tract.64,65 Mesonephric ducts are embryonic tubes that develop into the male reproductive organs; they regress in females during embryonic development, and remnants of these ducts may be located along the lateral walls of the vagina, cervix and adnexal structures.66 Despite their name, they are mostly likely of Müllerian origin and acquired mesonephric-like phenotype subsequently.67
Common architectural growth of mesonephric-like carcinomas include tubular, ductal, papillary, retiform, spindled and solid patterns, commonly with an admixture of different patterns in the same tumor.65 Eosinophilic colloid-like material may be identified in the luminal spaces. The tumor cells may display nuclear features resembling papillary thyroid carcinoma, including open chromatin and nuclear grooves.68 On immunohistochemistry, these tumors are positive for GATA3, TTF1 and CD10, with apical luminal staining in tubules.66 The extent of staining of these three markers is variable and morphology remains important. Mesonephric-like carcinoma usually shows minimal or absent expression of ER and PR, and wild-type expression of p53.64,68 They also demonstrate mismatch repair proficiency.69 Compared with other endometrial carcinomas, mesonephric-like carcinomas are more aggressive, with shorter progression-free survival (18.2 months vs 183 months for low-grade endometrioid carcinoma and 67.1 months for uterine serous carcinoma) and a higher risk of distant metastasis, including lung metastasis.68
Undifferentiated and dedifferentiated carcinomas of the uterine corpus
Undifferentiated carcinoma is defined as malignant epithelial neoplasm lacking overt lineage differentiation. Dedifferentiated carcinoma features both undifferentiated carcinoma and differentiated components.70 They account for 2% of endometrial carcinomas.70 More than half of patients with carcinomas containing undifferentiated components present at an advanced stage (Stage III–IV).71 A possible association with mismatch repair deficiency and Lynch syndrome has been suggested.72 Inactivating mutations involving chromatin remodeling genes (SMARCA4, SMARCB1, ARID1A and ARID1B) are found in two-thirds of dedifferentiated carcinomas and in half of undifferentiated carcinomas.73,74
The common histological features of undifferentiated carcinoma include solid growth with no nesting, glandular or trabecular architecture.75 The tumor cells are typically arranged in discohesive sheets with high mitotic activity. Rhabdoid morphology and focal myxoid matrix may be present.70 Dedifferentiated carcinoma consists of undifferentiated carcinoma and a differentiated component, most commonly low-grade endometrioid carcinoma (Figure 4B), though some cases are associated with high-grade endometrioid or serous carcinoma.76,77 A key differential diagnosis is high-grade endometrioid carcinoma, which may also show solid growth.70 Immunohistochemically, the undifferentiated carcinoma component in > 80% of tumors shows loss of epithelial and Müllerian differentiations, and is characterized by loss of or reduced expression in one or more cytokeratins and PAX-8;75 there is usually loss of E-cadherin staining, and mismatch repair proteins are lost in > 50% of cases.75,76 Abnormal overexpression of p53 is seen in 15–31% of cases.75,77 Loss of expression of SMARCA4 (BRG1), SMARCB1 (INI1), ARID1A or ARID1B occurs in approximately two-thirds of cases.77,78
Undifferentiated and dedifferentiated carcinomas are generally highly aggressive, with 55–95% of cases developing recurrence or resulting in death.70 Tumors with POLE hotspot mutations tend to have a more favorable prognosis, while those with mismatch repair deficiency have an intermediate outcome.78,79
Mixed carcinoma of the uterine corpus
Mixed carcinoma refers to endometrial carcinomas composed of two or more histological types, with at least one component being serous, clear cell or mesonephric-like.80 It is an uncommon tumor81 and large-scale epidemiological data are lacking. These tumors typically arise from progression or divergence from low-grade endometrioid carcinoma with a shared clonal origin.82,83 They often show mismatch repair protein deficiency84 and POLE hotspot mutations.85,86
Histologically, the different types must be spatially distinct, and variants of other endometrial carcinoma types or carcinosarcoma should be excluded before diagnosing mixed carcinoma.51,80 The most common combination is endometrioid and serous carcinoma, followed by endometrioid and clear cell carcinoma.80 A small proportion of serous or clear cell carcinoma within a mixed carcinoma may indicate an adverse prognosis.87,88 Any percentage of high-grade carcinoma that fits the histological and immunohistochemical features, admixed with low-grade endometrioid carcinoma, should be reported; such tumors are classified as mixed endometrial carcinoma.
The prognosis of mixed carcinoma is poorer than that of pure low-grade tumors, regardless of the percentage of high-grade component.88,89 They are graded as high-grade endometrial carcinomas. It remains uncertain whether mixed carcinomas confer a better prognosis than pure high-grade carcinomas.90,91 Cases with mismatch repair deficiency or POLE hotspot mutations are potentially associated with better prognosis.86
Other endometrial carcinomas
Primary endometrial squamous cell carcinoma
Primary endometrial squamous cell carcinoma is defined as endometrial carcinoma with exclusive squamous differentiation and no endometrioid component.65 It comprises < 1% of endometrial carcinomas and commonly occurs in postmenopausal women (average age, 67 years).92,93,94 It may be associated with chronic pyometra, nulliparity and ichthyosis uteri (keratinizing squamous metaplasia of endometrium), which may occur in the setting of uterine prolapse, pelvic radiotherapy or cervical stenosis.91 Most cases are not related to human papillomavirus.92,93,94 TP53 alterations may be identified. The histological features include infiltrating nests of squamous cells with keratinization; extensive sampling is required to exclude an underlying endometrioid carcinoma component.93 The prognosis is reported to be poor based on limited data.93,95
Gastric (gastrointestinal)-type endometrial carcinoma
Gastric (gastrointestinal)-type endometrial carcinoma exhibits gastric/gastrointestinal differentiation without a definite endometrioid component.65 Most cases occur in postmenopausal women (median age, 69 years),96,97 and > 60% are classified as p53-abnormal molecular subgroup.97 Clinical presentation may include mucoid vaginal discharge.96 The tumor typically shows gastrointestinal differentiation by histology (e.g. goblet cells, mucin pools and signet ring cells), and typical endometrioid glands should be absent.96,97,98 The background endometrium may display gastric-type mucinous metaplasia, which is a postulated precursor lesion.96,97,98 Diagnosis may be made when there is expression of neutral mucin as demonstrated by combined alcian blue-PAS stain, and immunohistochemistry including expression of HIK-1083, claudin 18.2, and loss of both ER and PR. This type of carcinoma is reported to behave aggressively, even at early stages with low-grade morphology, although no direct comparison with other types of endometrial carcinoma are available.96,97,98
Endometrial carcinoma with features resembling yolk sac tumors or choriocarcinomas
Endometrial carcinoma with features resembling yolk sac tumors or choriocarcinomas (or other germ cell/trophoblastic tumors) are classified as 'endometrial carcinoma with somatically derived germ cell/trophoblastic component'.65 These are rare (≤ 1%) and typically occur in postmenopausal women.99,100,101,102 Elevated serum alpha-fetoprotein (AFP) or human chorionic gonadotropin (hCG) may be seen.99,102 The germ cell or trophoblastic component share similar genetic mutations with Müllerian-type carcinomas, indicating a somatic origin.99,100 Histologically, the yolk sac component is commonly glandular or papillary, solid, reticular, microcystic or hepatoid, and commonly associated with extracellular basement membrane-like material. The cells lining glands and papillae are tall and columnar, and contain subnuclear and/or supranuclear cytoplasmic vacuoles (resembling primitive endoderm), irregular and enlarged nuclei with vesicular chromatin and prominent nucleoli. Cells in the reticular and solid patterns and those forming Schiller-Duval bodies, have a blastemal appearance and are characterized by a high nuclear/cytoplasmic ratio, with small, dark and hyperchromatic nuclei. The choriocarcinoma component is recognized by a bilaminar growth pattern of cytotrophoblasts and syncytiotrophoblastic giant cells. The background Müllerian type endometrial carcinoma may be endometrioid, serous, clear cell, dedifferentiated carcinomas or carcinosarcoma. Rare cases of pure germ cell or trophoblastic tumors may represent overgrowth of their pre-existing Müllerian type carcinoma.100,101,102 These tend to be aggressive and respond poorly to treatment.100 Recently, endometrial carcinoma with somatically derived yolk sac components have been shown to belong primarily to p53 abnormal molecular subgroup (> 70%), with smaller numbers as mismatch repair deficient and NSMP subgroups.102 Demonstration of HER2 overexpression in these tumors may provide an additional therapeutic option.102
Neuroendocrine carcinoma of the endometrium
Neuroendocrine carcinoma of the endometrium is characterized by features of small cell carcinoma.65 It accounts for < 1% of endometrial carcinomas,103 in women with a median age of 57 years.104 It may present with paraneoplastic syndrome such as retinopathy105 and Cushing syndrome due to ectopic ACTH secretion.106 The molecular profile is similar to that of conventional endometrial carcinomas, supporting a non-neuroendocrine origin.103,107 Histologically, these tumors resemble small cell neuroendocrine carcinomas of other organs, and often with a component of conventional endometrial carcinoma.103,104,107 Neuroendocrine markers (e.g. synaptophysin and chromogranin) should be present in at least 10% of tumor cells.65 This histotype is associated with a poor prognosis, with median survival around 17 months and 5-year survival of approximately 38%.108 Pure neuroendocrine carcinoma has a worse prognosis than that of mixed cases.109
Pilomatrix-like high-grade endometrioid carcinoma (PiMHEC)
Pilomatrix-like high-grade endometrioid carcinoma (PiMHEC) is a recently described, aggressive subtype of endometrial carcinoma. It affects postmenopausal women and is often at advanced FIGO stage at presentation. Histologically, the high-grade carcinoma comprises solid sheets or nests of basaloid to squamoid cells with severe pleomorphism, frequent mitoses and striking tumor necrosis. The defining feature is the presence of abundant ghost or shadow cells with keratinization closely mimicking cutaneous pilomatrix carcinoma. This tumor is often admixed with a low-grade endometrioid carcinoma. These tumors show reduced or loss of ER, PR and PAX8, and diffuse nuclear b-catenin expression. Most PiMHEC harbor CTNNB1 exon 3 mutations.110,111,112
Carcinosarcoma of the uterine corpus
Carcinosarcomas are defined as biphasic tumors with components of both high-grade carcinoma and sarcoma.51 They comprise approximately 5% of endometrial cancers, and most cases occur in postmenopausal women.113 Tamoxifen-related carcinosarcomas account for approximately 8% of uterine carcinosarcomas.114,115 Carcinosarcomas have also been reported as a potential long-term complication (> 5 years) following pelvic irradiation.116 The carcinomatous and sarcomatous components share similar genetic mutations, indicating a common cell of origin,117,118 with epithelial-mesenchymal transition playing a role;119 TP53 alterations are identified in 90% of cases117,118 and most cases are classified as p53-abnormal molecular subtype.
An admixture of malignant epithelial and mesenchymal components is characteristic of carcinosarcomas (Figure 4C). The carcinomatous component typically features endometrioid or serous differentiation, while the mesenchymal component is usually a high-grade sarcoma, with occasional heterologous differentiation (including rhabdomyosarcoma, chondrosarcoma and, rarely, osteosarcoma).51,118 Most (> 90%) metastases consist of carcinoma or carcinosarcoma, rather than pure sarcoma.118
The diagnosis of carcinosarcomas confers a poorer prognosis, as these tumors account for 30% of uterine cancer deaths.120 Early-stage disease (FIGO Stage I–II) shows a disease-specific survival rate of about 60% at 5 years, which decreases to less than 25% and 10% for Stages III and IV, respectively.121 The p53-abnormal and NSMP molecular subtypes are associated with worse prognosis, while POLE-ultramutated carcinomas tend to have excellent prognosis.122,123
BIOMARKER TESTING
Biomarker testing in endometrial carcinoma plays an important role in classification and determination of prognosis and treatment response7 The principal biomarkers and current recommendations for their use are detailed in Table 2. Figure 5 provides examples of immunohistochemical staining of these biomarkers.
2
Biomarkers for endometrial cancers.
Biomarker | Clinical implication | Current recommendation |
Hormone receptor: ER and PR | Expression predicts better prognosis in endometrioid carcinomas124,125,126 | Current NCCN guidelines recommend testing for ER and PR status in cases of advanced stage (Stage III–IV) or recurrent endometrioid endometrial carcinomas127 |
HER2 (human epidermal growth factor receptor 2) | HER2 protein overexpression is identified in approximately 35% of p53-abnormal endometrial carcinomas;128 to identify patients who may benefit from anti-HER2 agents | HER2 testing recommended by NCCN guidelines in cases with p53-abnormal endometrial carcinomas127 |
MMR (mismatch repair) proteins: MLH1, MSH2, MSH6, PMS2 | MMR-deficient tumors are more responsive to immune checkpoint inhibitor (dostarlimab or pembrolizumab) combined with standard chemotherapy129 | MMR immunohistochemistry testing is included in the diagnostic algorithm for molecular classification, as recommended by WHO,130 FIGO,19 CAP35and ESGO/ESTRO/ESP131 guidelines; MLH1 promotor methylation status may be performed in case of MLH1/PMS2 deficiency, and Lynch syndrome screening should be performed if no hypermethylation of MLH1 is found or in case of strong family history131 |
p53 protein (encoded by TP53) | Mutations are associated with the copy number–high molecular subtype, which has a poor prognosis;7 combined adjuvant chemotherapy and radiotherapy are recommended132 | p53 testing is part of molecular classification, suggested by WHO, FIGO and ESGO/ESTRO/ESP19,130,131 |
PD-L1 | Expression predicts better response to immune checkpoint inhibitors133 | PD-L1 may be considered in cases with normal MMR status35 |
CAP, College of American Pathologists; ER, estrogen receptor; FIGO, International Federation of Gynecology and Obstetrics; ESGO, European Society of Gynaecological Oncology; ESP, European Society of Pathologists; ESTRO, European Society of Radiotherapy and Oncology; NCCN, National Comprehensive Cancer Network; PR, progesterone receptor; WHO, World Health Organization.
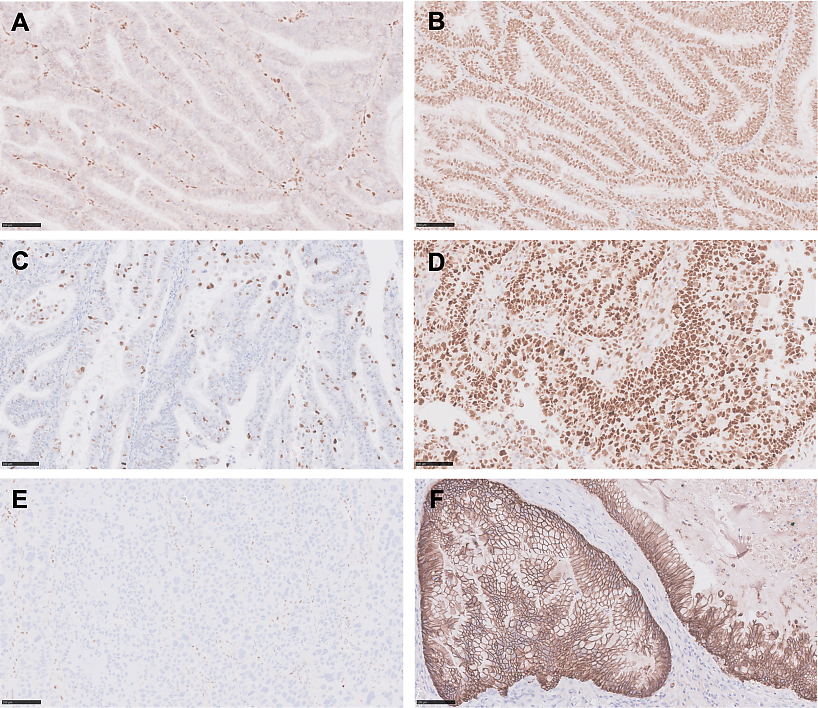
5
Immunohistochemistry of endometrial carcinoma biomarkers. (A) Loss of MLH1 nuclear staining in the tumor cells with intact expression in background stromal cells. (B) Intact nuclear expression of MSH2 in tumor cells. (C) Heterogeneous weak-to-moderate nuclear staining consistent with wild-type p53 expression. (D) Abnormal diffuse p53 overexpression in > 90% of tumor cell nuclei. (E) Abnormal null pattern of p53 with absence of nuclear staining in tumor cells and retained staining in background stromal cells. (F) Basolateral and circumferential membranous staining for HER2 (score 3+). Scale bar represents 100 μm.
STAGING
Endometrial carcinomas are staged according to the Union for International Cancer Control (UICC) TNM Classification (published in 2017) or FIGO staging.10 The latter was updated in 2023 (Appendix 1),19 replacing the staging system proposed in 2009 (Appendix 2).134
Stage-I and -II tumors represent tumors confined to the uterus and cervical stroma (except Stage IA3). Stage-III tumors show locoregional spread, while Stage-IV tumors involve spread to mucosa of non-gynecological organs and/or distant metastases.19 Changes from the 2009 FIGO staging system include the integration of molecular classification; notably, the status of POLE and p53 mutations influences prognosis for tumors confined to the uterine corpus. Tumors with POLE mutation are classified as Stage IAmPOLEmut, while those with abnormal p53 status are assigned a high stage (Stage IICmp53abn).19
Pathological parameters essential for staging, applicable to all endometrial carcinomas include:
- Histological type: tumors are classified into non-aggressive types (Grade 1 and 2 endometrioid endometrial carcinomas) and aggressive types (serous, clear cell, undifferentiated and dedifferentiated carcinoma, carcinosarcoma, mesonephric-like carcinoma, neuroendocrine carcinoma, endometrial carcinoma with somatically derived germ cell components, gastric/gastrointestinal-type endometrial carcinoma, high-grade endometrioid carcinoma and pilomatrix-like high-grade endometrioid carcinoma)
- FIGO histological grade: low (FIGO Grades 1 and 2) and high (FIGO Grade 3)
- Myometrial invasion: ≥ 50% myometrial invasion is a prognostic risk factor135
- Lymphovascular space invasion (LVSI): should be assessed at the invasive front;19,136,137 substantial LVSI (defined by ≥ 5 LVSI) and cervical/endocervical LVSI are associated with worse survival compared to focal LVSI (< 5 LVSI)137
- Lower uterine segment involvement: linked to higher risk of distant metastasis or death;136,138 patients with Lynch syndrome more frequently have involvement of this segment139
- Cervical stromal invasion: defined as tumor destruction of endocervical fibrous stroma
- Adnexal involvement: synchronous low-grade tumors of the endometrium and ovary are associated with good prognosis;10,140 Stage IA3 is reserved for low-grade synchronous endometrioid carcinoma composed of unilateral ovarian tumor without capsular extension, and endometrial tumor without deep (≥ 50%) myometrial invasion, substantial LVSI or additional metastases19
- Uterine serosal involvement (a Stage IIIA2 disease)
- Lymph node status: sentinel lymph node ultrastaging (sectioning of lymph node in 2 mm intervals) is recommended
- Molecular subtypes
CONCLUSION
Endometrial cancer is a common malignancy with rising incidence, particularly among postmenopausal women. Advances in histological and molecular classification have improved prognostic stratification, aiding therapeutic decision-making.141 Ongoing research aims to discover new, clinically significant biomarkers, and refining staging systems that are globally applicable.
PRACTICE RECOMMENDATIONS
- Incorporating histological and molecular features into endometrial carcinoma classification improves diagnostic accuracy and prognosis prediction in regions with available resources.10
- Molecular classification can alter the management of endometrial carcinomas.21
- A binary grading system is recommended for biopsy and curettage specimens when surgical staging is planned; distinguishing Grades 1 and 2 remains important for fertility-sparing therapeutic approaches.21
- Patients diagnosed with mismatch repair-deficient endometrial carcinoma should proceed to MLH1 promoter methylation if there is MLH1 and PMS2 loss on immunohistochemistry. In the absence of MLH1 promoter hypermethylation, patients should be referred to counseling for Lynch syndrome screening.24,138
- Biomarker testing should include ER, PR, p53, MLH1, MSH2, MSH6, and PMS2. HER2 should be added to p53-abnormal endometrial carcinoma, and scoring should be done according to the most recent College of American Pathologists guidelines.35
CONFLICTS OF INTEREST
The author(s) of this chapter declare that they have no interests that conflict with the contents of the chapter.
Feedback
Publishers’ note: We are constantly trying to update and enhance chapters in this Series. So if you have any constructive comments about this chapter please provide them to us by selecting the "Your Feedback" link in the left-hand column.
APPENDIX 1
2023 FIGO staging of cancer of the endometrium19
Stage | Description | |||
Stage I | Confined to the uterine corpus and ovary | |||
IA | Disease limited to the endometrium OR non-aggressive histological type, i.e. low-grade endometrioid, with invasion of less than half of myometrium with no or focal lymphovascular space involvement (LVSI) OR good prognosis disease | |||
IA1 | Non-aggressive histological type limited to an endometrial polyp OR confined to the endometrium | |||
IA2 | Non-aggressive histological types involving less than half of the myometrium with no or focal LVSI | |||
IA3 | Low-grade endometrioid carcinomas limited to the uterus and ovarya | |||
IB | Non-aggressive histological types with invasion of half or more of the myometrium, and with no or focal LVSI | |||
IC | Aggressive histological types limited to a polyp or confined to the endometrium | |||
Stage II | Invasion of cervical stroma without extrauterine extension OR with substantial LVSI OR aggressive histological types with myometrial invasion | |||
IIA | Invasion of the cervical stroma of non-aggressive histological types | |||
IIB | Substantial LVSI of non-aggressive histological types | |||
IIC | Aggressive histological types with any myometrial involvement | |||
Stage III | Local and/or regional spread of the tumor of any histological subtype | |||
IIIA | Invasion of uterine serosa, adnexa or both by direct extension or metastasis | |||
IIIA1 | Spread to ovary or Fallopian tube (except when meeting Stage IA3 criteria)a | |||
IIIA2 | Involvement of uterine subserosa or spread through the uterine serosa | |||
IIIB | Metastasis or direct spread to the vagina and/or to the parametrium or pelvic peritoneum | |||
IIIB1 | Metastasis or direct spread to the vagina and/or the parametrium | |||
IIIB2 | Metastasis to the pelvic peritoneum | |||
IIIC | Metastasis to the pelvic or para-aortic lymph nodes or bothb | |||
IIIC1 | Metastasis to the pelvic lymph nodes | |||
IIIC1i | Micrometastasis | |||
IIIC1ii | Macrometastasis | |||
IIIC2 | Metastasis to para-aortic lymph nodes up to the renal vessels, with or without metastasis to the pelvic lymph nodes | |||
IIIC2i | Micrometastasis | |||
IIIC2i | Macrometastasis | |||
Stage IV | Spread to the bladder mucosa and/or intestinal mucosa and/or distant metastasis | |||
IVA | Invasion of the bladder mucosa and/or the intestinal/bowel mucosa | |||
IVB | Abdominal peritoneal metastasis beyond the pelvis | |||
IVC | Distant metastasis, including metastasis to any extra- or intra-abdominal lymph nodes above the renal vessels, lungs, liver, brain, or bone | |||
- Disease limited to low-grade endometrioid carcinomas involving the endometrium and ovaries (Stage IA3) should fulfill the following criteria:
- no more than superficial myometrial invasion (< 50%)
- absence of extensive/substantial LVSI
- absence of additional metastases
- the ovarian tumor is unilateral, limited to the ovary, without capsule invasion/rupture (equivalent to pT1a).
- Micrometastasis: > 2 mm in size; macrometastasis (0.2–2 mm and/or > 200 cells)
FIGO endometrial cancer stage with molecular classification19
Stage | Molecular findings in patients with early endometrial cancer (Stages I and II after surgical staging) |
Stage IAmPOLEmut | POLEmut endometrial carcinoma, confined to the uterine corpus or with cervical extension, regardless of the degree of LVSI or histological type |
Stage IICmp53abn | p53abn endometrial carcinoma confined to the uterine corpus with any myometrial invasion, with or without cervical invasion, and regardless of the degree of LVSI or histological type |
APPENDIX 2
Revised FIGO 2009 staging system134
Stage | Description | ||
Stage I | Tumor confined to the uterine corpus | ||
IA | No or less than half myometrial invasion | ||
IB | Invasion to or more than half of the myometrium | ||
Stage II | Tumor invades cervical stroma, but does not extend beyond the uterus | ||
Stage III | Local and/or regional spread of the tumor | ||
IIIA | Tumor invades the serosa and/or adnexa | ||
IIIB | Vaginal and/or parametrial involvement | ||
IIIC | Metastases to the pelvic and/or para-aortic lymph nodes | ||
| IIIC1 | Positive pelvic nodes | ||
| IIIC2 | Positive para-aortic lymph nodes with or without positive pelvic lymph nodes | ||
Stage IV | Tumor invades bladder and/or bowel mucosa, and/or distant metastases | ||
IVA | Tumor invades bladder and/or bowel mucosa | ||
IVB | Distant metastases, including intra-abdominal metastases and/or inguinal lymph nodes | ||
REFERENCES
Liu L, Habeshian TS, Zhang J, Peeri NC, Du M, De Vivo I, Setiawan VW. Differential trends in rising endometrial cancer incidence by age, race, and ethnicity. JNCI Cancer Spectr. 2023;7(1). doi: 10.1093/jncics/pkad001. PubMed PMID: 36625534; PMCID: PMC9904185. | |
Mahdy H, Vadakekut ES, Crotzer D. Endometrial Cancer. [Updated 2024 Apr 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK525981/. | |
Lortet-Tieulent J, Ferlay J, Bray F, Jemal A. International Patterns and Trends in Endometrial Cancer Incidence, 1978–2013. J Natl Cancer Inst. 2018;110(4):354–361. doi: 10.1093/jnci/djx214. PubMed PMID: 29045681. | |
Gu B, Shang X, Yan M, Li X, Wang W, Wang Q, Zhang C. Variations in incidence and mortality rates of endometrial cancer at the global, regional, and national levels, 1990–2019. Gynecol Oncol. 2021;161(2):573–580. Epub 20210205. doi: 10.1016/j.ygyno.2021.01.036. PubMed PMID: 33551200. | |
Gordhandas S, Zammarrelli WA, Rios-Doria EV, Green AK, Makker V. Current Evidence-Based Systemic Therapy for Advanced and Recurrent Endometrial Cancer. J Natl Compr Canc Netw. 2023;21(2):217–226. doi: 10.6004/jnccn.2022.7254. PubMed PMID: 36791759; PMCID: PMC10361357. | |
Matias-Guiu X, Oliva E, McCluggage WG, Nucci M, Longacre TA. Tumours of the uterine corpus: Introduction. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. p. 243. | |
Kandoth C, Schultz N, Cherniack AD, Akbani R, Liu Y, Shen H, Robertson AG, Pashtan I, Shen R, Benz CC, Yau C, Laird PW, Ding L, Zhang W, Mills GB, Kucherlapati R, Mardis ER, Levine DA. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73. doi: 10.1038/nature12113. PubMed PMID: 23636398; PMCID: PMC3704730. | |
Matsuo K, Mandelbaum RS, Matsuzaki S, Klar M, Roman LD, Wright JD. Ovarian conservation for young women with early-stage, low-grade endometrial cancer: a 2-step schema. Am J Obstet Gynecol. 2021;224(6):574–584. Epub 20210104. doi: 10.1016/j.ajog.2020.12.1213. PubMed PMID: 33412129. | |
Clarke MA, Long BJ, Del Mar Morillo A, Arbyn M, Bakkum-Gamez JN, Wentzensen N. Association of Endometrial Cancer Risk With Postmenopausal Bleeding in Women: A Systematic Review and Meta-analysis. JAMA Intern Med. 2018;178(9):1210–1222. doi: 10.1001/jamainternmed.2018.2820. PubMed PMID: 30083701; PMCID: PMC6142981. | |
Bosse T, Davidson B, Singh N, Euscher ED, Raspollini MR, Liu C, Lortet-Tieulent J. Endometrioid carcinoma of the uterine corpus. In: Matias-Guiu X, Lax S, editors. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. p. 252–256. | |
Gilks CB, Oliva E, Soslow RA. Poor interobserver reproducibility in the diagnosis of high-grade endometrial carcinoma. Am J Surg Pathol. 2013;37(6):874–881. doi: 10.1097/PAS.0b013e31827f576a. PubMed PMID: 23629444. | |
Hoang LN, McConechy MK, Köbel M, Han G, Rouzbahman M, Davidson B, Irving J, Ali RH, Leung S, McAlpine JN, Oliva E, Nucci MR, Soslow RA, Huntsman DG, Gilks CB, Lee CH. Histotype-genotype correlation in 36 high-grade endometrial carcinomas. Am J Surg Pathol. 2013;37(9):1421–1432. doi: 10.1097/PAS.0b013e31828c63ed. PubMed PMID: 24076778. | |
Clement PB, Young RH. Endometrioid carcinoma of the uterine corpus: a review of its pathology with emphasis on recent advances and problematic aspects. Adv Anat Pathol. 2002;9(3):145–184. doi: 10.1097/00125480-200205000-00001. PubMed PMID: 11981113. | |
Clement PB, Young RH. Non-endometrioid carcinomas of the uterine corpus: a review of their pathology with emphasis on recent advances and problematic aspects. Adv Anat Pathol. 2004;11(3):117–142. doi: 10.1097/00125480-200405000-00001. PubMed PMID: 15096727. | |
World Health Organization. International histological classification of tumours: histological typing of female genital tract tumours. Geneva: World Health Organization; 1973. | |
Scully RE, Bonfiglio TA, Kurman RJ, Silverberg SG, Wilkinson EJ. Histological typing of female genital tract tumours. 2nd ed. Berlin: Springer-Verlag; 1994. | |
Tavassoli FAD, P. Pathology & Genetics of Tumours of the Breast and Female Genital Organs. 3rd Edition ed. Lyon, France: International Agency for Research on Cancer Press; 2003. | |
Kurman RJC, Maria Luisa; Herrington, C. Simon; Young, Robert H. WHO Classification of Tumours of Female Reproductive Organs. 4th Edition ed. Lyon, France: International Agency for Research on Cancer; 2014. | |
Berek JS, Matias-Guiu X, Creutzberg C, Fotopoulou C, Gaffney D, Kehoe S, Lindemann K, Mutch D, Concin N. FIGO staging of endometrial cancer: 2023. J Gynecol Oncol. 2023;34(5):e85. Epub 20230808. doi: 10.3802/jgo.2023.34.e85. PubMed PMID: 37593813; PMCID: PMC10482588. | |
Helpman L, Kupets R, Covens A, Saad RS, Khalifa MA, Ismiil N, Ghorab Z, Dubé V, Nofech-Mozes S. Assessment of endometrial sampling as a predictor of final surgical pathology in endometrial cancer. Br J Cancer. 2014;110(3):609–615. Epub 20131224. doi: 10.1038/bjc.2013.766. PubMed PMID: 24366295; PMCID: PMC3915129. | |
Soslow RA, Tornos C, Park KJ, Malpica A, Matias-Guiu X, Oliva E, Parkash V, Carlson J, McCluggage WG, Gilks CB. Endometrial Carcinoma Diagnosis: Use of FIGO Grading and Genomic Subcategories in Clinical Practice: Recommendations of the International Society of Gynecological Pathologists. Int J Gynecol Pathol. 2019;38 Suppl 1(Iss 1 Suppl 1):S64–s74. doi: 10.1097/pgp.0000000000000518. PubMed PMID: 30550484; PMCID: PMC6295928. | |
Talhouk A, McConechy MK, Leung S, Li-Chang HH, Kwon JS, Melnyk N, Yang W, Senz J, Boyd N, Karnezis AN, Huntsman DG, Gilks CB, McAlpine JN. A clinically applicable molecular-based classification for endometrial cancers. Br J Cancer. 2015;113(2):299–310. Epub 20150630. doi: 10.1038/bjc.2015.190. PubMed PMID: 26172027; PMCID: PMC4506381. | |
Bosse T, Nout RA, McAlpine JN, McConechy MK, Britton H, Hussein YR, Gonzalez C, Ganesan R, Steele JC, Harrison BT, Oliva E, Vidal A, Matias-Guiu X, Abu-Rustum NR, Levine DA, Gilks CB, Soslow RA. Molecular Classification of Grade 3 Endometrioid Endometrial Cancers Identifies Distinct Prognostic Subgroups. Am J Surg Pathol. 2018;42(5):561–568. doi: 10.1097/pas.0000000000001020. PubMed PMID: 29505428; PMCID: PMC5893364. | |
Cho KR, Cooper K, Croce S, Djordevic B, Herrington S, Howitt B, Hui P, Ip P, Koebel M, Lax S, Quade BJ, Shaw P, Vidal A, Yemelyanova A, Clarke B, Hedrick Ellenson L, Longacre TA, Shih IM, McCluggage WG, Malpica A, Oliva E, Parkash V, Matias-Guiu X. International Society of Gynecological Pathologists (ISGyP) Endometrial Cancer Project: Guidelines From the Special Techniques and Ancillary Studies Group. Int J Gynecol Pathol. 2019;38 Suppl 1(Iss 1 Suppl 1):S114–s22. doi: 10.1097/pgp.0000000000000496. PubMed PMID: 29521846; PMCID: PMC6296838. | |
TCGA. Uterine corpus endometrial carcinoma (The Cancer Genome Atlas Research Network, PanCancer Atlas): cBioPortal for Cancer Genomics; 2013 [August 22, 2025]. Available from: https://www.cbioportal.org/study/summary?id=ucec_tcga_pub ] | |
Rayner E, van Gool IC, Palles C, Kearsey SE, Bosse T, Tomlinson I, Church DN. A panoply of errors: polymerase proofreading domain mutations in cancer. Nat Rev Cancer. 2016;16(2):71–81. doi: 10.1038/nrc.2015.12. PubMed PMID: 26822575. | |
Palles C, Cazier JB, Howarth KM, Domingo E, Jones AM, Broderick P, Kemp Z, Spain SL, Guarino E, Salguero I, Sherborne A, Chubb D, Carvajal-Carmona LG, Ma Y, Kaur K, Dobbins S, Barclay E, Gorman M, Martin L, Kovac MB, Humphray S, Lucassen A, Holmes CC, Bentley D, Donnelly P, Taylor J, Petridis C, Roylance R, Sawyer EJ, Kerr DJ, Clark S, Grimes J, Kearsey SE, Thomas HJ, McVean G, Houlston RS, Tomlinson I. Germline mutations affecting the proofreading domains of POLE and POLD1 predispose to colorectal adenomas and carcinomas. Nat Genet. 2013;45(2):136–144. Epub 20121223. doi: 10.1038/ng.2503. PubMed PMID: 23263490; PMCID: PMC3785128. | |
Hussein YR, Weigelt B, Levine DA, Schoolmeester JK, Dao LN, Balzer BL, Liles G, Karlan B, Köbel M, Lee CH, Soslow RA. Clinicopathological analysis of endometrial carcinomas harboring somatic POLE exonuclease domain mutations. Mod Pathol. 2015;28(4):505–514. Epub 20141114. doi: 10.1038/modpathol.2014.143. PubMed PMID: 25394778. | |
Van Gool IC, Ubachs JEH, Stelloo E, de Kroon CD, Goeman JJ, Smit V, Creutzberg CL, Bosse T. Blinded histopathological characterisation of POLE exonuclease domain-mutant endometrial cancers: sheep in wolf's clothing. Histopathology. 2018;72(2):248–258. Epub 20171010. doi: 10.1111/his.13338. PubMed PMID: 28795426. | |
Ryan NAJ, Glaire MA, Blake D, Cabrera-Dandy M, Evans DG, Crosbie EJ. The proportion of endometrial cancers associated with Lynch syndrome: a systematic review of the literature and meta-analysis. Genet Med. 2019;21(10):2167–2180. Epub 20190514. doi: 10.1038/s41436-019-0536-8. PubMed PMID: 31086306; PMCID: PMC8076013. | |
Loukovaara M, Pasanen A, Bützow R. Mismatch Repair Deficiency as a Predictive and Prognostic Biomarker in Molecularly Classified Endometrial Carcinoma. Cancers (Basel). 2021;13(13). Epub 20210622. doi: 10.3390/cancers13133124. PubMed PMID: 34206702; PMCID: PMC8268938. | |
Watkins JC, Nucci MR, Ritterhouse LL, Howitt BE, Sholl LM. Unusual Mismatch Repair Immunohistochemical Patterns in Endometrial Carcinoma. Am J Surg Pathol. 2016;40(7):909–916. doi: 10.1097/pas.0000000000000663. PubMed PMID: 27186853. | |
Mendoza RP, Wang P, Schulte JJ, Tjota MY, Jani I, Martinez AC, Haridas R, Wanjari P, Steinhardt G, Brown N, Betz BL, Chapel DB, Kertowidjojo E, Yamada SD, Bennett JA. Endometrial Carcinomas With Subclonal Loss of Mismatch Repair Proteins: A Clinicopathologic and Genomic Study. Am J Surg Pathol. 2023;47(5):589–598. Epub 20230303. doi: 10.1097/pas.0000000000002031. PubMed PMID: 36866757. | |
Shia J, Black D, Hummer AJ, Boyd J, Soslow RA. Routinely assessed morphological features correlate with microsatellite instability status in endometrial cancer. Hum Pathol. 2008;39(1):116–125. Epub 20071018. doi: 10.1016/j.humpath.2007.05.022. PubMed PMID: 17949789. | |
Turashvili G, Karnezis AN, Hulkower KI, Hebert C, Harik L, Crothers B, Giannico G, Deeb KK, Hanley K, Ganesan R, Mills A, Buza N. Reporting Results of Biomarker Testing of Specimens From Patients With Carcinoma of Gynecologic Origin: The Updated College of American Pathologists Protocol. Arch Pathol Lab Med. 2025. Epub 20250916. doi: 10.5858/arpa.2025-0157-CP. PubMed PMID: 40956279. | |
Garg K, Leitao MM, Jr., Wynveen CA, Sica GL, Shia J, Shi W, Soslow RA. p53 overexpression in morphologically ambiguous endometrial carcinomas correlates with adverse clinical outcomes. Mod Pathol. 2010;23(1):80–92. Epub 20091023. doi: 10.1038/modpathol.2009.153. PubMed PMID: 19855378. | |
Jamieson A, Vermij L, Kramer CJH, Jobsen JJ, Jürgemlienk-Schulz I, Lutgens L, Mens JW, Haverkort MAD, Slot A, Nout RA, Oosting J, Carlson J, Howitt BE, Ip PPC, Lax SF, McCluggage WG, Singh N, McAlpine JN, Creutzberg CL, Horeweg N, Gilks CB, Bosse T. Clinical Behavior and Molecular Landscape of Stage I p53-Abnormal Low-Grade Endometrioid Endometrial Carcinomas. Clin Cancer Res. 2023;29(23):4949–4957. doi: 10.1158/1078-0432.Ccr-23-1397. PubMed PMID: 37773079; PMCID: PMC10690141. | |
Vermij L, Jobsen JJ, León-Castillo A, Brinkhuis M, Roothaan S, Powell ME, de Boer SM, Khaw P, Mileshkin LR, Fyles A, Leary A, Genestie C, Jürgenliemk-Schulz IM, Crosbie EJ, Mackay HJ, Nijman HW, Nout RA, Smit V, Creutzberg CL, Horeweg N, Bosse T. Prognostic refinement of NSMP high-risk endometrial cancers using oestrogen receptor immunohistochemistry. Br J Cancer. 2023;128(7):1360–1368. Epub 20230123. doi: 10.1038/s41416-023-02141-0. PubMed PMID: 36690721; PMCID: PMC10050005. | |
Thompson EF, Huvila J, Jamieson A, Leung S, Lum A, Offman S, Lytwyn A, Sur ML, Hoang L, Irving J, van der Westhuizen N, Morin C, Bicamumpaka C, Azordegan N, Gougeon F, Ennour-Idrissi K, Senz J, McConechy MK, Aguirre-Hernandez R, Lui V, Kuo C, Bell C, Salisbury T, Lawson J, He E, Wang S, Chiu D, Kean S, Samouëlian V, Salvador S, Gotlieb W, Helpman L, Scott S, Wohlmuth C, Vicus D, Plante M, Talhouk A, Huntsman D, Parra-Herran C, Kinloch M, Grondin K, Gilks CB, McAlpine JN. Variability in endometrial carcinoma pathology practice: opportunities for improvement with molecular classification. Mod Pathol. 2022;35(12):1974–1982. Epub 20221014. doi: 10.1038/s41379-022-01165-w. PubMed PMID: 36241860. | |
Piulats JM, Guerra E, Gil-Martín M, Roman-Canal B, Gatius S, Sanz-Pamplona R, Velasco A, Vidal A, Matias-Guiu X. Molecular approaches for classifying endometrial carcinoma. Gynecol Oncol. 2017;145(1):200–207. Epub 20161229. doi: 10.1016/j.ygyno.2016.12.015. PubMed PMID: 28040204. | |
Rabban JT, Gilks CB, Malpica A, Matias-Guiu X, Mittal K, Mutter GL, Oliva E, Parkash V, Ronnett BM, Staats P, Stewart CJR, McCluggage WG. Issues in the Differential Diagnosis of Uterine Low-grade Endometrioid Carcinoma, Including Mixed Endometrial Carcinomas: Recommendations from the International Society of Gynecological Pathologists. Int J Gynecol Pathol. 2019;38 Suppl 1(Iss 1 Suppl 1):S25–s39. doi: 10.1097/pgp.0000000000000512. PubMed PMID: 30550482; PMCID: PMC6296831. | |
Malpica A. How to approach the many faces of endometrioid carcinoma. Mod Pathol. 2016;29 Suppl 1:S29–44. doi: 10.1038/modpathol.2015.142. PubMed PMID: 26715172. | |
Fader AN, Boruta D, Olawaiye AB, Gehrig PA. Uterine papillary serous carcinoma: epidemiology, pathogenesis and management. Curr Opin Obstet Gynecol. 2010;22(1):21–29. doi: 10.1097/GCO.0b013e328334d8a3. PubMed PMID: 19952744. | |
Hui P, Kelly M, O'Malley DM, Tavassoli F, Schwartz PE. Minimal uterine serous carcinoma: a clinicopathological study of 40 cases. Mod Pathol. 2005;18(1):75–82. doi: 10.1038/modpathol.3800271. PubMed PMID: 15389257. | |
Bland AE, Calingaert B, Secord AA, Lee PS, Valea FA, Berchuck A, Soper JT, Havrilesky L. Relationship between tamoxifen use and high risk endometrial cancer histologic types. Gynecol Oncol. 2009;112(1):150–154. Epub 20081019. doi: 10.1016/j.ygyno.2008.08.035. PubMed PMID: 18937966. | |
Pothuri B, Ramondetta L, Eifel P, Deavers MT, Wilton A, Alektiar K, Barakat R, Soslow RA. Radiation-associated endometrial cancers are prognostically unfavorable tumors: a clinicopathologic comparison with 527 sporadic endometrial cancers. Gynecol Oncol. 2006;103(3):948–951. Epub 20060725. doi: 10.1016/j.ygyno.2006.05.039. PubMed PMID: 16870239. | |
Matanes E, Volodarsky-Perel A, Eisenberg N, Rottenstreich M, Yasmeen A, Mitric C, Lau S, Salvador S, Gotlieb WH, Kogan L. Endometrial Cancer in Germline BRCA Mutation Carriers: A Systematic Review and Meta-analysis. J Minim Invasive Gynecol. 2021;28(5):947–956. Epub 20201127. doi: 10.1016/j.jmig.2020.11.023. PubMed PMID: 33249269. | |
Schultheis AM, Martelotto LG, De Filippo MR, Piscuglio S, Ng CK, Hussein YR, Reis-Filho JS, Soslow RA, Weigelt B. TP53 Mutational Spectrum in Endometrioid and Serous Endometrial Cancers. Int J Gynecol Pathol. 2016;35(4):289–300. doi: 10.1097/pgp.0000000000000243. PubMed PMID: 26556035; PMCID: PMC5087968. | |
Fadare O, Stewart C. Clear cell carcinoma of the uterine corpus. In: Matias-Guiu X, Lax S, editors. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. p. 258. | |
Irshaid L, Costigan DC, Dong F, Matulonis UA, Nucci MR, Kolin DL. Molecular Landscape of Mullerian Clear Cell Carcinomas Identifies The Cancer Genome Atlas-like Prognostic Subgroups. Mod Pathol. 2023;36(5):100123. Epub 20230204. doi: 10.1016/j.modpat.2023.100123. PubMed PMID: 36857998. | |
Palacios P, Ali-Fehmi R, Carlson J. Carcinosarcoma of the uterine corpus. In: Matias-Guiu X, Lax S, editors. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. p. 266. | |
Ellenson L, Stewart C, Parkash V. Serous carcinoma of the uterine corpus. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. | |
Buza N, English DP, Santin AD, Hui P. Toward standard HER2 testing of endometrial serous carcinoma: 4-year experience at a large academic center and recommendations for clinical practice. Mod Pathol. 2013;26(12):1605–1612. Epub 20130614. doi: 10.1038/modpathol.2013.113. PubMed PMID: 23765245. | |
Fader AN, Roque DM, Siegel E, Buza N, Hui P, Abdelghany O, Chambers SK, Secord AA, Havrilesky L, O'Malley DM, Backes F, Nevadunsky N, Edraki B, Pikaart D, Lowery W, ElSahwi KS, Celano P, Bellone S, Azodi M, Litkouhi B, Ratner E, Silasi DA, Schwartz PE, Santin AD. Randomized Phase II Trial of Carboplatin-Paclitaxel Versus Carboplatin-Paclitaxel-Trastuzumab in Uterine Serous Carcinomas That Overexpress Human Epidermal Growth Factor Receptor 2/neu. J Clin Oncol. 2018;36(20):2044–2051. Epub 20180327. doi: 10.1200/jco.2017.76.5966. PubMed PMID: 29584549. | |
Bernardini MQ, Gien LT, Lau S, Altman AD, Gilks B, Ferguson SE, Köbel M, Samouëlian V, Wesa M, Cameron A, Nelson G, Han G, Clarke B, Ho TC, Panzarella T, Atenafu EG, McAlpine JN. Treatment related outcomes in high-risk endometrial carcinoma: Canadian high risk endometrial cancer consortium (CHREC). Gynecol Oncol. 2016;141(1):148–154. Epub 20160205. doi: 10.1016/j.ygyno.2016.02.002. PubMed PMID: 26854651. | |
Zannoni GF, Santoro A, Angelico G, Spadola S, Arciuolo D, Valente M, Inzani F, Pettinato A, Vatrano S, Fanfani F, Scambia G, Fraggetta F. Clear cell carcinoma of the endometrium: an immunohistochemical and molecular analysis of 45 cases. Hum Pathol. 2019;92:10–17. Epub 20190630. doi: 10.1016/j.humpath.2019.06.005. PubMed PMID: 31269413. | |
Nigon E, Lefeuvre-Plesse C, Martinez A, Chauleur C, Lortholary A, Favier L, Bats AS, Guille A, AdélaÏde J, Finetti P, de Casteljac V, Provansal M, Mamessier E, Bertucci F, Ray-Coquard I, Sabatier R. Clinical, pathological, and comprehensive molecular analysis of the uterine clear cell carcinoma: a retrospective national study from TMRG and GINECO network. J Transl Med. 2023;21(1):408. Epub 20230623. doi: 10.1186/s12967-023-04264-7. PubMed PMID: 37353806; PMCID: PMC10288685. | |
Fadare O, Zheng W, Crispens MA, Jones HW, Khabele D, Gwin K, Liang SX, Mohammed K, Desouki MM, Parkash V, Hecht JL. Morphologic and other clinicopathologic features of endometrial clear cell carcinoma: a comprehensive analysis of 50 rigorously classified cases. Am J Cancer Res. 2013;3(1):70–95. Epub 20130118. PubMed PMID: 23359866; PMCID: PMC3555196. | |
Murali R, Davidson B, Fadare O, Carlson JA, Crum CP, Gilks CB, Irving JA, Malpica A, Matias-Guiu X, McCluggage WG, Mittal K, Oliva E, Parkash V, Rutgers JKL, Staats PN, Stewart CJR, Tornos C, Soslow RA. High-grade Endometrial Carcinomas: Morphologic and Immunohistochemical Features, Diagnostic Challenges and Recommendations. Int J Gynecol Pathol. 2019;38 Suppl 1(Iss 1 Suppl 1):S40–s63. doi: 10.1097/pgp.0000000000000491. PubMed PMID: 30550483; PMCID: PMC6296248. | |
Han G, Soslow RA, Wethington S, Levine DA, Bogomolniy F, Clement PB, Köbel M, Gilks B, DeLair D. Endometrial Carcinomas With Clear Cells: A Study of a Heterogeneous Group of Tumors Including Interobserver Variability, Mutation Analysis, and Immunohistochemistry With HNF-1β. Int J Gynecol Pathol. 2015;34(4):323–333. doi: 10.1097/pgp.0000000000000162. PubMed PMID: 25851704. | |
Travaglino A, Raffone A, Santoro A, Raimondo D, Angelico G, Valente M, Arciuolo D, Scaglione G, D'Alessandris N, Casadio P, Inzani F, Mollo A, Seracchioli R, Zannoni GF. Clear cell endometrial carcinomas with mismatch repair deficiency have a favorable prognosis: A systematic review and meta-analysis. Gynecol Oncol. 2021;162(3):804–808. Epub 20210712. doi: 10.1016/j.ygyno.2021.07.007. PubMed PMID: 34266691. | |
Na K, Kim HS. Clinicopathologic and Molecular Characteristics of Mesonephric Adenocarcinoma Arising From the Uterine Body. Am J Surg Pathol. 2019;43(1):12–25. doi: 10.1097/pas.0000000000000991. PubMed PMID: 29189288; PMCID: PMC6296843. | |
Pors J, Segura S, Chiu DS, Almadani N, Ren H, Fix DJ, Howitt BE, Kolin D, McCluggage WG, Mirkovic J, Gilks B, Park KJ, Hoang L. Clinicopathologic Characteristics of Mesonephric Adenocarcinomas and Mesonephric-like Adenocarcinomas in the Gynecologic Tract: A Multi-institutional Study. Am J Surg Pathol. 2021;45(4):498–506. doi: 10.1097/pas.0000000000001612. PubMed PMID: 33165093; PMCID: PMC7954854. | |
Kim HG, Kim H, Yeo MK, Won KY, Kim YS, Han GH, Kim HS, Na K. Mesonephric-like Adenocarcinoma of the Uterine Corpus: Comprehensive Analyses of Clinicopathological, Molecular, and Prognostic Characteristics With Retrospective Review of 237 Endometrial Carcinoma Cases. Cancer Genomics Proteomics. 2022;19(4):526–539. doi: 10.21873/cgp.20338. PubMed PMID: 35732320; PMCID: PMC9247884. | |
Singh N, Hoang L, Ip Pea. Other endometrial carcinomas. In: matias-Guiu X, Lax S, editors. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. p. 276. | |
Howitt BE, Emori MM, Drapkin R, Gaspar C, Barletta JA, Nucci MR, McCluggage WG, Oliva E, Hirsch MS. GATA3 Is a Sensitive and Specific Marker of Benign and Malignant Mesonephric Lesions in the Lower Female Genital Tract. Am J Surg Pathol. 2015;39(10):1411–1419. doi: 10.1097/pas.0000000000000471. PubMed PMID: 26135559. | |
Mirkovic J, Olkhov-Mitsel E, Amemiya Y, Al-Hussaini M, Nofech-Mozes S, Djordjevic B, Kupets R, Seth A, McCluggage WG. Mesonephric-like adenocarcinoma of the female genital tract: novel observations and detailed molecular characterisation of mixed tumours and mesonephric-like carcinosarcomas. Histopathology. 2023;82(7):978–990. Epub 20230331. doi: 10.1111/his.14892. PubMed PMID: 36860193. | |
Euscher ED, Bassett R, Duose DY, Lan C, Wistuba I, Ramondetta L, Ramalingam P, Malpica A. Mesonephric-like Carcinoma of the Endometrium: A Subset of Endometrial Carcinoma With an Aggressive Behavior. Am J Surg Pathol. 2020;44(4):429–243. doi: 10.1097/pas.0000000000001401. PubMed PMID: 31725471. | |
Kim H, Kim HS. Mesonephric-like Adenocarcinoma of the Uterine Corpus: Comparison Between Mismatch Repair Protein Immunostaining and Microsatellite Instability Testing. Anticancer Res. 2023;43(4):1785–1795. doi: 10.21873/anticanres.16332. PubMed PMID: 36974792. | |
Palacios J, Ramalingam P, Lee C. Undifferentiated and dedifferentiated carcinomas of the uterine corpus. In: Matias-Guiu X, Lax S, editors. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. p. 262. | |
Tafe LJ, Garg K, Chew I, Tornos C, Soslow RA. Endometrial and ovarian carcinomas with undifferentiated components: clinically aggressive and frequently underrecognized neoplasms. Mod Pathol. 2010;23(6):781–789. Epub 20100319. doi: 10.1038/modpathol.2010.41. PubMed PMID: 20305618. | |
Rosa-Rosa JM, Leskelä S, Cristóbal-Lana E, Santón A, López-García M, Muñoz G, Pérez-Mies B, Biscuola M, Prat J, Esther O, Soslow RA, Matias-Guiu X, Palacios J. Molecular genetic heterogeneity in undifferentiated endometrial carcinomas. Mod Pathol. 2016;29(11):1390–1398. Epub 20160805. doi: 10.1038/modpathol.2016.132. PubMed PMID: 27491810; PMCID: PMC5708881. | |
Köbel M, Hoang LN, Tessier-Cloutier B, Meng B, Soslow RA, Stewart CJR, Lee CH. Undifferentiated Endometrial Carcinomas Show Frequent Loss of Core Switch/Sucrose Nonfermentable Complex Proteins. Am J Surg Pathol. 2018;42(1):76–83. doi: 10.1097/pas.0000000000000941. PubMed PMID: 28863077; PMCID: PMC7995487. | |
Karnezis AN, Hoang LN, Coatham M, Ravn S, Almadani N, Tessier-Cloutier B, Irving J, Meng B, Li X, Chow C, McAlpine J, Kuo KT, Mao TL, Djordjevic B, Soslow RA, Huntsman DG, Blake Gilks C, Köbel M, Lee CH. Loss of switch/sucrose non-fermenting complex protein expression is associated with dedifferentiation in endometrial carcinomas. Mod Pathol. 2016;29(3):302–314. Epub 20160108. doi: 10.1038/modpathol.2015.155. PubMed PMID: 26743474; PMCID: PMC4980656. | |
Ramalingam P, Masand RP, Euscher ED, Malpica A. Undifferentiated Carcinoma of the Endometrium: An Expanded Immunohistochemical Analysis Including PAX-8 and Basal-Like Carcinoma Surrogate Markers. Int J Gynecol Pathol. 2016;35(5):410–418. doi: 10.1097/pgp.0000000000000248. PubMed PMID: 26598976. | |
Busca A, Parra-Herran C, Nofech-Mozes S, Djordjevic B, Ismiil N, Cesari M, Nucci MR, Mirkovic J. Undifferentiated endometrial carcinoma arising in the background of high-grade endometrial carcinoma – Expanding the definition of dedifferentiated endometrial carcinoma. Histopathology. 2020;77(5):769–780. Epub 20200927. doi: 10.1111/his.14186. PubMed PMID: 32557836. | |
Olkhov-Mitsel E, Busca A, Parra-Herran C, Amemiya Y, Nofech-Mozes S, Djordjevic B, Nucci MR, Seth A, Mirkovic J. Genomic profiling of dedifferentiated endometrial carcinomas arising in the background of high-grade carcinoma: a targeted next-generation sequencing study. Histopathology. 2023;83(3):366–375. Epub 20230524. doi: 10.1111/his.14938. PubMed PMID: 37222195. | |
Shin CY, Gokbayrak B, Tao VL, Almadani N, E SL, Ho R, Kommoss FK, Huvila J, Chiu D, Leung S, Tessier-Cloutier B, Huntsman DG, Gilks CB, McAlpine JN, Hoang L, Wang Y. Prognostic values of molecular subtypes and SWI/SNF protein expression in de-differentiated/undifferentiated endometrial carcinoma. Histopathology. 2025;86(7):1053–1063. Epub 20250115. doi: 10.1111/his.15411. PubMed PMID: 39811899; PMCID: PMC12045760. | |
Hammer PM, Wang A, Vermij L, Zdravkovic S, Heilbroner L, Ryan E, Geisick RLP, Charu V, Longacre TA, Suarez CJ, Ho C, Jenkins TM, Mills AM, Bosse T, Howitt BE. Molecular Classification Outperforms Histologic Classification in Prognostication of High-grade Endometrial Carcinomas With Undifferentiated and Sarcomatous Components. Am J Surg Pathol. 2024;48(8):953–964. Epub 20240523. doi: 10.1097/pas.0000000000002250. PubMed PMID: 38780000. | |
Parkash V, Rabban J, Katabuchi H. Mixed carcinoma of the uterine corpus. In: Matias-Guiu X, Lax S, editors. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. p. 272. | |
Lawrenson K, Pakzamir E, Liu B, Lee JM, Delgado MK, Duncan K, Gayther SA, Liu S, Roman L, Mhawech-Fauceglia P. Molecular Analysis of Mixed Endometrioid and Serous Adenocarcinoma of the Endometrium. PLoS One. 2015;10(7):e0130909. Epub 20150701. doi: 10.1371/journal.pone.0130909. PubMed PMID: 26132201; PMCID: PMC4488511. | |
Matrai C, Motanagh S, Mirabelli S, Ma L, He B, Chapman-Davis E, Kurtis B, Elemento O, Mosquera JM, Ellenson LH. Molecular Profiles of Mixed Endometrial Carcinoma. Am J Surg Pathol. 2020;44(8):1104–1111. doi: 10.1097/pas.0000000000001519. PubMed PMID: 32604171. | |
Köbel M, Meng B, Hoang LN, Almadani N, Li X, Soslow RA, Gilks CB, Lee CH. Molecular Analysis of Mixed Endometrial Carcinomas Shows Clonality in Most Cases. Am J Surg Pathol. 2016;40(2):166–180. doi: 10.1097/pas.0000000000000536. PubMed PMID: 26492180; PMCID: PMC5029122. | |
Köbel M, Tessier-Cloutier B, Leo J, Hoang LN, Gilks CB, Soslow RA, Delair D, Stewart CJR, Lee CH. Frequent Mismatch Repair Protein Deficiency in Mixed Endometrioid and Clear Cell Carcinoma of the Endometrium. Int J Gynecol Pathol. 2017;36(6):555–561. doi: 10.1097/pgp.0000000000000369. PubMed PMID: 28114191. | |
Haight PJ, Esnakula A, Riedinger CJ, Suarez AA, Gillespie J, Patton A, Chassen A, Cohn DE, Cosgrove CM. Molecular characterization of mixed-histology endometrial carcinoma provides prognostic and therapeutic value over morphologic findings. NPJ Precis Oncol. 2025;9(1):41. Epub 20250208. doi: 10.1038/s41698-025-00803-1. PubMed PMID: 39922938; PMCID: PMC11807167. | |
Conlon N, Da Cruz Paula A, Ashley CW, Segura S, De Brot L, da Silva EM, Soslow RA, Weigelt B, DeLair DF. Endometrial Carcinomas with a "Serous" Component in Young Women Are Enriched for DNA Mismatch Repair Deficiency, Lynch Syndrome, and POLE Exonuclease Domain Mutations. Am J Surg Pathol. 2020;44(5):641–648. doi: 10.1097/pas.0000000000001461. PubMed PMID: 32205482; PMCID: PMC7156312. | |
Quddus MR, Sung CJ, Zhang C, Lawrence WD. Minor serous and clear cell components adversely affect prognosis in ''mixed-type'' endometrial carcinomas: a clinicopathologic study of 36 stage-I cases. Reprod Sci. 2010;17(7):673–678. Epub 20100414. doi: 10.1177/1933719110368433. PubMed PMID: 20393071. | |
Li W, Li L, Wu M, Lang J, Bi Y. The Prognosis of Stage IA Mixed Endometrial Carcinoma. Am J Clin Pathol. 2019;152(5):616–624. doi: 10.1093/ajcp/aqz083. PubMed PMID: 31318970. | |
Hagemann IS, Deng W, Zaino RJ, Powell MA, Gunderson C, Cosgrove C, Mathews C, Pearl ML, Waggoner S, Ghebre R, Lele S, Guntupalli S, Secord AA, Ioffe O, Park K, Rasty G, Singh M, Soslow R, Creasman W, Mutch DG. The presence of an endometrioid component does not alter the clinicopathologic profile or survival of patients with uterine serous cancer: A gynecologic oncology group (GOG/NRG) study of 934 women. Gynecol Oncol. 2021;160(3):660–668. Epub 20210108. doi: 10.1016/j.ygyno.2020.12.040. PubMed PMID: 33423806; PMCID: PMC8188294. | |
Hagemann IS, Deng W, Zaino RJ, Powell MA, Gunderson Jackson C, Cosgrove C, Mathews C, Pearl ML, Waggoner S, Ghebre R, Lele S, Guntupalli S, Secord AA, Ioffe O, Rasty G, Singh M, Soslow R, Creasman W, Mutch DG. Mixed clear cell/endometrioid and clear cell/serous carcinoma of the uterus are clinicopathologically similar to pure clear cell carcinoma: An NRG Oncology/Gynecologic Oncology Group (GOG-210) study of 311 women. Gynecol Oncol. 2023;177:38–45. Epub 20230825. doi: 10.1016/j.ygyno.2023.08.005. PubMed PMID: 37634258; PMCID: PMC10806844. | |
Reijnen C, Vrede SW, Eijkelenboom A, Draak R, Sweegers S, Snijders M, van Gestel P, Pijnenborg JMA, Bulten J, Küsters-Vandevelde HVN. Pure and mixed clear cell carcinoma of the endometrium: A molecular and immunohistochemical analysis study. Cancer Med. 2023;12(11):12365–12376. Epub 20230420. doi: 10.1002/cam4.5937. PubMed PMID: 37081760; PMCID: PMC10278528. | |
Goodman A, Zukerberg LR, Rice LW, Fuller AF, Young RH, Scully RE. Squamous cell carcinoma of the endometrium: a report of eight cases and a review of the literature. Gynecol Oncol. 1996;61(1):54–60. doi: 10.1006/gyno.1996.0096. PubMed PMID: 8626118. | |
Hopkins MR, Palsgrove DN, Ronnett BM, Vang R, Lin J, Murdock TA. Molecular Analysis of HPV-independent Primary Endometrial Squamous Cell Carcinoma Reveals TP53 and CDKN2A Comutations : A Clinicopathologic Analysis With Re-evaluation of Diagnostic Criteria. Am J Surg Pathol. 2022;46(12):1611–1622. Epub 20220905. doi: 10.1097/pas.0000000000001970. PubMed PMID: 36069815. | |
Bures N, Nelson G, Duan Q, Magliocco A, Demetrick D, Duggan MA. Primary squamous cell carcinoma of the endometrium: clinicopathologic and molecular characteristics. Int J Gynecol Pathol. 2013;32(6):566–575. doi: 10.1097/PGP.0b013e31828cb0be. PubMed PMID: 24071873. | |
Li JJX, Ip PPC. Endometrial Cancer: An Update on Prognostic Pathologic Features and Clinically Relevant Biomarkers. Surg Pathol Clin. 2022;15(2):277–299. doi: 10.1016/j.path.2022.02.006. PubMed PMID: 35715162. | |
Wong RW, Talia KL, McCluggage WG. Gastric-type glandular lesions of the female genital tract excluding the cervix: emerging pathological entities. Histopathology. 2024;85(1):20–39. Epub 20240313. doi: 10.1111/his.15174. PubMed PMID: 38477341. | |
Kaur H, Lin LH, Kolin DL, Pinto A, Parra-Herran C, Catherwood M, Van de Vijver K, Buza N, McCluggage WG, Nucci MR. Primary Endometrial Gastric (Gastrointestinal)-type Mucinous Adenocarcinoma: A Detailed Clinicopathologic and Molecular Analysis of 27 Cases. Am J Surg Pathol. 2025;49(6):564–577. Epub 20250311. doi: 10.1097/pas.0000000000002382. PubMed PMID: 40066786. | |
Wong RW, Ralte A, Grondin K, Talia KL, McCluggage WG. Endometrial Gastric (Gastrointestinal)-type Mucinous Lesions: Report of a Series Illustrating the Spectrum of Benign and Malignant Lesions. Am J Surg Pathol. 2020;44(3):406–419. doi: 10.1097/pas.0000000000001381. PubMed PMID: 31567280. | |
Skala SL, Liu CJ, Udager AM, Sciallis AP. Molecular characterization of uterine and ovarian tumors with mixed epithelial and germ cell features confirms frequent somatic derivation. Mod Pathol. 2020;33(10):1989–2000. Epub 20200513. doi: 10.1038/s41379-020-0548-6. PubMed PMID: 32404953. | |
Acosta AM, Sholl LM, Cin PD, Howitt BE, Otis CN, Nucci MR. Malignant tumours of the uterus and ovaries with Mullerian and germ cell or trophoblastic components have a somatic origin and are characterised by genomic instability(). Histopathology. 2020;77(5):788–797. Epub 20200922. doi: 10.1111/his.14188. PubMed PMID: 32558949. | |
Mills AM, Jenkins TM, Dibbern ME, Atkins KA, Ring KL. Yolk Sac Differentiation in Endometrial Carcinoma: Incidence and Clinicopathologic Features of Somatically Derived Yolk Sac Tumors Versus Carcinomas With Nonspecific Immunoexpression of Yolk Sac Markers. Am J Surg Pathol. 2024;48(7):790–802. Epub 20240423. doi: 10.1097/pas.0000000000002230. PubMed PMID: 38651612. | |
Li JJX, Chui MH, McCluggage WG, Fadare O, Cheng GHW, Ko JMK, Dungog CC, Lee JHS, Ma ESK, Tse KY, Ip PPC. Endometrial Carcinomas With a Somatically-derived Yolk Sac Tumor Component Share Molecular Similarities to p53-abnormal Endometrial Carcinomas and Germ Cell Tumors. Mod Pathol. 2026:100976. Epub 20260212. doi: 10.1016/j.modpat.2026.100976. PubMed PMID: 41690477. | |
Howitt BE, Dong F, Vivero M, Shah V, Lindeman N, Schoolmeester JK, Baltay M, MacConaill L, Sholl LM, Nucci MR, McCluggage WG. Molecular Characterization of Neuroendocrine Carcinomas of the Endometrium: Representation in All 4 TCGA Groups. Am J Surg Pathol. 2020;44(11):1541–1548. doi: 10.1097/pas.0000000000001560. PubMed PMID: 32773531. | |
Pocrnich CE, Ramalingam P, Euscher ED, Malpica A. Neuroendocrine Carcinoma of the Endometrium: A Clinicopathologic Study of 25 Cases. Am J Surg Pathol. 2016;40(5):577–586. doi: 10.1097/pas.0000000000000633. PubMed PMID: 26945341; PMCID: PMC5998806. | |
Ju W, Park IA, Kim SH, Lee SE, Kim SC. Small cell carcinoma of the uterine corpus manifesting with visual dysfunction. Gynecol Oncol. 2005;99(2):504–506. Epub 20050819. doi: 10.1016/j.ygyno.2005.06.045. PubMed PMID: 16112716. | |
Sato H, Kanai G, Kajiwara H, Itoh J, Osamura RY. Small-cell carcinoma of the endometrium presenting as Cushing's syndrome. Endocr J. 2010;57(1):31–38. Epub 20091016. doi: 10.1507/endocrj.k09e-212. PubMed PMID: 19834252. | |
Ono K, Kasajima R, Katayama K, Miyagi Y, Yokose T. Clinicopathological and molecular characteristics of endometrial neuroendocrine carcinomas reveal preexisting endometrial carcinoma origin. Pathol Int. 2021;71(8):491–499. Epub 20210520. doi: 10.1111/pin.13108. PubMed PMID: 34015161. | |
Schlechtweg K, Chen L, St Clair CM, Tergas AI, Khoury-Collado F, Hou JY, Melamed A, Neugut AI, Hershman DL, Wright JD. Neuroendocrine carcinoma of the endometrium: Disease course, treatment, and outcomes. Gynecol Oncol. 2019;155(2):254–261. Epub 20190910. doi: 10.1016/j.ygyno.2019.09.004. PubMed PMID: 31519319. | |
Matsumoto H, Shimokawa M, Nasu K, Shikama A, Shiozaki T, Futagami M, Kai K, Nagano H, Mori T, Yano M, Sugino N, Fujimoto E, Yoshioka N, Nakagawa S, Shimada M, Tokunaga H, Yamada Y, Tsuruta T, Tasaki K, Nishikawa R, Kuji S, Motohashi T, Ito K, Yamada T, Teramoto N. Clinicopathologic features, treatment, prognosis and prognostic factors of neuroendocrine carcinoma of the endometrium: a retrospective analysis of 42 cases from the Kansai Clinical Oncology Group/Intergroup study in Japan. J Gynecol Oncol. 2019;30(6):e103. doi: 10.3802/jgo.2019.30.e103. PubMed PMID: 31576694; PMCID: PMC6779616. | |
Zhou F, Qin L, Huang S, Lin W, Zhang H, Parkash V, Zheng W. Pilomatrix-like High-grade Endometrial Carcinoma: An Underdiagnosed Entity With Aggressive Clinicopathologic Features. Am J Surg Pathol. 2025;49(8):818–829. Epub 20250409. doi: 10.1097/pas.0000000000002402. PubMed PMID: 40202384. | |
Xu J, Park KJ, Weisman PS. An Expanded Series of Pilomatrix-like High-grade Endometrioid Carcinoma (PiMHEC), Including Both MMR Deficient and MMR Proficient Cases. Int J Gynecol Pathol. 2024;43(1):67–69. Epub 20230505. doi: 10.1097/pgp.0000000000000955. PubMed PMID: 37192144; PMCID: PMC10625643. | |
Weisman P, Park KJ, Xu J. FIGO Grade 3 Endometrioid Adenocarcinomas With Diffusely Aberrant β-Catenin Expression: An Aggressive Subset Resembling Cutaneous Pilomatrix Carcinomas. Int J Gynecol Pathol. 2022;41(2):126–131. doi: 10.1097/pgp.0000000000000775. PubMed PMID: 33811207; PMCID: PMC8484367. | |
Matsuo K, Ross MS, Machida H, Blake EA, Roman LD. Trends of uterine carcinosarcoma in the United States. J Gynecol Oncol. 2018;29(2):e22. Epub 20180105. doi: 10.3802/jgo.2018.29.e22. PubMed PMID: 29400015; PMCID: PMC5823983. | |
McCluggage WG, Abdulkader M, Price JH, Kelehan P, Hamilton S, Beattie J, Al-Nafussi A. Uterine carcinosarcomas in patients receiving tamoxifen. A report of 19 cases. Int J Gynecol Cancer. 2000;10(4):280–284. doi: 10.1046/j.1525-1438.2000.010004280.x. PubMed PMID: 11240687. | |
Matsuo K, Ross MS, Bush SH, Yunokawa M, Blake EA, Takano T, Ueda Y, Baba T, Satoh S, Shida M, Ikeda Y, Adachi S, Yokoyama T, Takekuma M, Takeuchi S, Nishimura M, Iwasaki K, Yanai S, Klobocista MM, Johnson MS, Machida H, Hasegawa K, Miyake TM, Nagano T, Pejovic T, Shahzad MM, Im DD, Omatsu K, Ueland FR, Kelley JL, Roman LD. Tumor characteristics and survival outcomes of women with tamoxifen-related uterine carcinosarcoma. Gynecol Oncol. 2017;144(2):329–335. Epub 20161205. doi: 10.1016/j.ygyno.2016.11.042. PubMed PMID: 27931750; PMCID: PMC7526046. | |
Wakayama A, Kudaka W, Nakasone T, Taira Y, Aoki Y. Secondary uterine carcinosarcoma after concurrent chemoradiotherapy for cervical cancer: Case reports. Gynecol Oncol Rep. 2017;21:81–83. Epub 20170717. doi: 10.1016/j.gore.2017.07.008. PubMed PMID: 28761924; PMCID: PMC5524167. | |
McConechy MK, Hoang LN, Chui MH, Senz J, Yang W, Rozenberg N, Mackenzie R, McAlpine JN, Huntsman DG, Clarke BA, Gilks CB, Lee CH. In-depth molecular profiling of the biphasic components of uterine carcinosarcomas. J Pathol Clin Res. 2015;1(3):173–185. Epub 20150409. doi: 10.1002/cjp2.18. PubMed PMID: 27499902; PMCID: PMC4939881. | |
Gotoh O, Sugiyama Y, Takazawa Y, Kato K, Tanaka N, Omatsu K, Takeshima N, Nomura H, Hasegawa K, Fujiwara K, Taki M, Matsumura N, Noda T, Mori S. Clinically relevant molecular subtypes and genomic alteration-independent differentiation in gynecologic carcinosarcoma. Nat Commun. 2019;10(1):4965. Epub 20191031. doi: 10.1038/s41467-019-12985-x. PubMed PMID: 31672974; PMCID: PMC6823358. | |
Cherniack AD, Shen H, Walter V, Stewart C, Murray BA, Bowlby R, Hu X, Ling S, Soslow RA, Broaddus RR, Zuna RE, Robertson G, Laird PW, Kucherlapati R, Mills GB, Weinstein JN, Zhang J, Akbani R, Levine DA. Integrated Molecular Characterization of Uterine Carcinosarcoma. Cancer Cell. 2017;31(3):411–423. doi: 10.1016/j.ccell.2017.02.010. PubMed PMID: 28292439; PMCID: PMC5599133. | |
Matsuo K, Takazawa Y, Ross MS, Elishaev E, Podzielinski I, Yunokawa M, Sheridan TB, Bush SH, Klobocista MM, Blake EA, Takano T, Matsuzaki S, Baba T, Satoh S, Shida M, Nishikawa T, Ikeda Y, Adachi S, Yokoyama T, Takekuma M, Fujiwara K, Hazama Y, Kadogami D, Moffitt MN, Takeuchi S, Nishimura M, Iwasaki K, Ushioda N, Johnson MS, Yoshida M, Hakam A, Li SW, Richmond AM, Machida H, Mhawech-Fauceglia P, Ueda Y, Yoshino K, Yamaguchi K, Oishi T, Kajiwara H, Hasegawa K, Yasuda M, Kawana K, Suda K, Miyake TM, Moriya T, Yuba Y, Morgan T, Fukagawa T, Wakatsuki A, Sugiyama T, Pejovic T, Nagano T, Shimoya K, Andoh M, Shiki Y, Enomoto T, Sasaki T, Fujiwara K, Mikami M, Shimada M, Konishi I, Kimura T, Post MD, Shahzad MM, Im DD, Yoshida H, Omatsu K, Ueland FR, Kelley JL, Karabakhtsian RG, Roman LD. Significance of histologic pattern of carcinoma and sarcoma components on survival outcomes of uterine carcinosarcoma. Ann Oncol. 2016;27(7):1257–1266. Epub 20160406. doi: 10.1093/annonc/mdw161. PubMed PMID: 27052653. | |
Gonzalez Bosquet J, Terstriep SA, Cliby WA, Brown-Jones M, Kaur JS, Podratz KC, Keeney GL. The impact of multi-modal therapy on survival for uterine carcinosarcomas. Gynecol Oncol. 2010;116(3):419–423. Epub 20091105. doi: 10.1016/j.ygyno.2009.10.053. PubMed PMID: 19896181. | |
Travaglino A, Raffone A, Raimondo D, Arciuolo D, Angelico G, Valente M, Scaglione G, D'Alessandris N, Casadio P, Inzani F, Mollo A, Santoro A, Seracchioli R, Franco Zannoni G. Prognostic value of the TCGA molecular classification in uterine carcinosarcoma. Int J Gynaecol Obstet. 2022;158(1):13–20. Epub 20211011. doi: 10.1002/ijgo.13937. PubMed PMID: 34536971; PMCID: PMC9292561. | |
Hammer PM, Momeni-Boroujeni A, Kolin DL, Kingsley L, Folkins A, Geisick RLP, Ho C, Suarez CJ, Howitt BE. POLE-Mutated Uterine Carcinosarcomas: A Clinicopathologic and Molecular Study of 11 Cases. Mod Pathol. 2025;38(3):100676. Epub 20241129. doi: 10.1016/j.modpat.2024.100676. PubMed PMID: 39615841. | |
Guan J, Xie L, Luo X, Yang B, Zhang H, Zhu Q, Chen X. The prognostic significance of estrogen and progesterone receptors in grade I and II endometrioid endometrial adenocarcinoma: hormone receptors in risk stratification. J Gynecol Oncol. 2019;30(1):e13. Epub 20181029. doi: 10.3802/jgo.2019.30.e13. PubMed PMID: 30479097; PMCID: PMC6304404. | |
Backes FJ, Walker CJ, Goodfellow PJ, Hade EM, Agarwal G, Mutch D, Cohn DE, Suarez AA. Estrogen receptor-alpha as a predictive biomarker in endometrioid endometrial cancer. Gynecol Oncol. 2016;141(2):312–317. Epub 20160310. doi: 10.1016/j.ygyno.2016.03.006. PubMed PMID: 26957478; PMCID: PMC4878441. | |
Trovik J, Wik E, Werner HM, Krakstad C, Helland H, Vandenput I, Njolstad TS, Stefansson IM, Marcickiewicz J, Tingulstad S, Staff AC, Amant F, Akslen LA, Salvesen HB. Hormone receptor loss in endometrial carcinoma curettage predicts lymph node metastasis and poor outcome in prospective multicentre trial. Eur J Cancer. 2013;49(16):3431–3441. Epub 20130808. doi: 10.1016/j.ejca.2013.06.016. PubMed PMID: 23932335. | |
Abu-Rustum N, Yashar C, Arend R, Barber E, Bradley K, Brooks R, Campos SM, Chino J, Chon HS, Chu C, Crispens MA, Damast S, Fisher CM, Frederick P, Gaffney DK, Giuntoli R, Han E, Holmes J, Howitt BE, Lea J, Mariani A, Mutch D, Nagel C, Nekhlyudov L, Podoll M, Salani R, Schorge J, Siedel J, Sisodia R, Soliman P, Ueda S, Urban R, Wethington SL, Wyse E, Zanotti K, McMillian NR, Aggarwal S. Uterine Neoplasms, Version 1.2023, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2023;21(2):181–209. doi: 10.6004/jnccn.2023.0006. PubMed PMID: 36791750. | |
Balestra A, Larsimont D, Noël JC. HER2 Amplification in p53-Mutated Endometrial Carcinomas. Cancers (Basel). 2023;15(5). Epub 20230224. doi: 10.3390/cancers15051435. PubMed PMID: 36900227; PMCID: PMC10001224. | |
Mirza MR, Chase DM, Slomovitz BM, dePont Christensen R, Novák Z, Black D, Gilbert L, Sharma S, Valabrega G, Landrum LM, Hanker LC, Stuckey A, Boere I, Gold MA, Auranen A, Pothuri B, Cibula D, McCourt C, Raspagliesi F, Shahin MS, Gill SE, Monk BJ, Buscema J, Herzog TJ, Copeland LJ, Tian M, He Z, Stevens S, Zografos E, Coleman RL, Powell MA. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. N Engl J Med. 2023;388(23):2145–2158. Epub 20230327. doi: 10.1056/NEJMoa2216334. PubMed PMID: 36972026. | |
Bosse T, Davidson B, Euscher Eea. Endometrioid carcinoma of the uterine corpus. Female Genital Tumours. 5th edition ed. Lyon (France): International Agency for Research on Cancer; 2020. | |
Concin N, Matias-Guiu X, Vergote I, Cibula D, Mirza MR, Marnitz S, Ledermann J, Bosse T, Chargari C, Fagotti A, Fotopoulou C, Gonzalez Martin A, Lax S, Lorusso D, Marth C, Morice P, Nout RA, O'Donnell D, Querleu D, Raspollini MR, Sehouli J, Sturdza A, Taylor A, Westermann A, Wimberger P, Colombo N, Planchamp F, Creutzberg CL. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12–39. Epub 20201218. doi: 10.1136/ijgc-2020-002230. PubMed PMID: 33397713. | |
León-Castillo A, de Boer SM, Powell ME, Mileshkin LR, Mackay HJ, Leary A, Nijman HW, Singh N, Pollock PM, Bessette P, Fyles A, Haie-Meder C, Smit V, Edmondson RJ, Putter H, Kitchener HC, Crosbie EJ, de Bruyn M, Nout RA, Horeweg N, Creutzberg CL, Bosse T. Molecular Classification of the PORTEC-3 Trial for High-Risk Endometrial Cancer: Impact on Prognosis and Benefit From Adjuvant Therapy. J Clin Oncol. 2020;38(29):3388–3397. Epub 20200804. doi: 10.1200/jco.20.00549. PubMed PMID: 32749941; PMCID: PMC7527156. | |
Santoro A, Angelico G, Inzani F, Arciuolo D, d'Amati A, Addante F, Travaglino A, Scaglione G, D'Alessandris N, Valente M, Tinnirello G, Raffone A, Narducci N, Piermattei A, Cianfrini F, Bragantini E, Zannoni GF. The emerging and challenging role of PD-L1 in patients with gynecological cancers: An updating review with clinico-pathological considerations. Gynecol Oncol. 2024;184:57–66. Epub 20240130. doi: 10.1016/j.ygyno.2024.01.032. PubMed PMID: 38295614. | |
Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105(2):103–104. doi: 10.1016/j.ijgo.2009.02.012. PubMed PMID: 19367689. | |
Creasman WT, Morrow CP, Bundy BN, Homesley HD, Graham JE, Heller PB. Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer. 1987;60(8 Suppl):2035–2041. doi: 10.1002/1097-0142(19901015)60:8+<2035::aid-cncr2820601515>3.0.co;2-8. PubMed PMID: 3652025. | |
Singh N, Hirschowitz L, Zaino R, Alvarado-Cabrero I, Duggan MA, Ali-Fehmi R, Euscher E, Hecht JL, Horn LC, Ioffe O, Matias-Guiu X, McCluggage WG, Mikami Y, Ordi J, Parkash V, Quddus MR, Quick CM, Staebler A, Zaloudek C, Nucci M, Malpica A, Oliva E. Pathologic Prognostic Factors in Endometrial Carcinoma (Other Than Tumor Type and Grade). Int J Gynecol Pathol. 2019;38 Suppl 1(Iss 1 Suppl 1):S93–s113. doi: 10.1097/pgp.0000000000000524. PubMed PMID: 30550486; PMCID: PMC6296841. | |
Ates D, Karahan S, Oruç A, Usubutun A. Lymphovascular Space Invasion in Endometrial Cancer: Does it Matter Where and How Much to Sample? A Macroscopic Study of 208 Hysterectomies. Mod Pathol. 2025;38(12):100885. Epub 20250911. doi: 10.1016/j.modpat.2025.100885. PubMed PMID: 40939816. | |
Matias-Guiu XA, L; Buza, N; Ellenson, LH; Fadare, O; Ganesan, R; Ip, PPC; Palacios, J; Raspollini, MR; Werner, HMJ; Lax, SF; McCluggage, WG. Endometrial Cancer Histopathology Reporting Guide. 5th edition. Sydney, Australia: International Collaboration on Cancer Reporting; 2024. Available from: https://www.iccr-cancer.org/datasets/published-datasets/female-reproductive/endometrial/ | |
Zhao S, Chen L, Zang Y, Liu W, Liu S, Teng F, Xue F, Wang Y. Endometrial cancer in Lynch syndrome. Int J Cancer. 2022;150(1):7–17. Epub 20210909. doi: 10.1002/ijc.33763. PubMed PMID: 34398969. | |
Turashvili G, Gómez-Hidalgo NR, Flynn J, Gonen M, Leitao MM, Jr., Soslow RA, Murali R. Risk-based stratification of carcinomas concurrently involving the endometrium and ovary. Gynecol Oncol. 2019;152(1):38–45. Epub 20181106. doi: 10.1016/j.ygyno.2018.10.033. PubMed PMID: 30413340; PMCID: PMC6321787. | |
Galant N, Krawczyk P, Monist M, Obara A, Gajek ?, Grenda A, Nico? M, Kalinka E, Milanowski J. Molecular Classification of Endometrial Cancer and Its Impact on Therapy Selection. Int J Mol Sci. 2024;25(11). Epub 20240528. doi: 10.3390/ijms25115893. PubMed PMID: 38892080; PMCID: PMC11172295. |
Online Study Assessment Option
All readers who are qualified doctors or allied medical professionals can automatically receive 2 Continuing Professional Development points plus a Study Completion Certificate from GLOWM for successfully answering four multiple-choice questions (randomly selected) based on the study of this chapter. Medical students can receive the Study Completion Certificate only.
(To find out more about the Continuing Professional Development awards program CLICK HERE)